
Apolipoprotein B (ApoB): The Single Best Marker for Cardiovascular Risk
Your doctor says your LDL cholesterol is 120 mg/dL—perfectly “normal.” Your calculated 10-year cardiovascular risk is 6%—”low-intermediate.” You’re told to exercise more and come back next year.
Meanwhile, your apolipoprotein B is 105 mg/dL—indicating you have significantly more atherogenic particles than your LDL number suggests. Your true cardiovascular risk is substantially higher than standard testing reveals.
This scenario plays out thousands of times daily in medical offices across the country. Standard lipid panels measure cholesterol content. ApoB counts actual atherogenic particles. In approximately 20-30% of people, these markers tell dramatically different stories. When they disagree, ApoB is the better predictor of who actually has heart attacks and strokes.
As longevity physician Peter Attia consistently emphasizes, if you can only measure one lipid-related marker for cardiovascular risk assessment, ApoB is the one to choose. It’s the most accurate, most direct measurement of atherogenic particle burden available in standard clinical practice.
High performers don’t make cardiovascular risk decisions based on incomplete data. They measure what actually matters—particle number, not just cholesterol content.
What Is Apolipoprotein B?
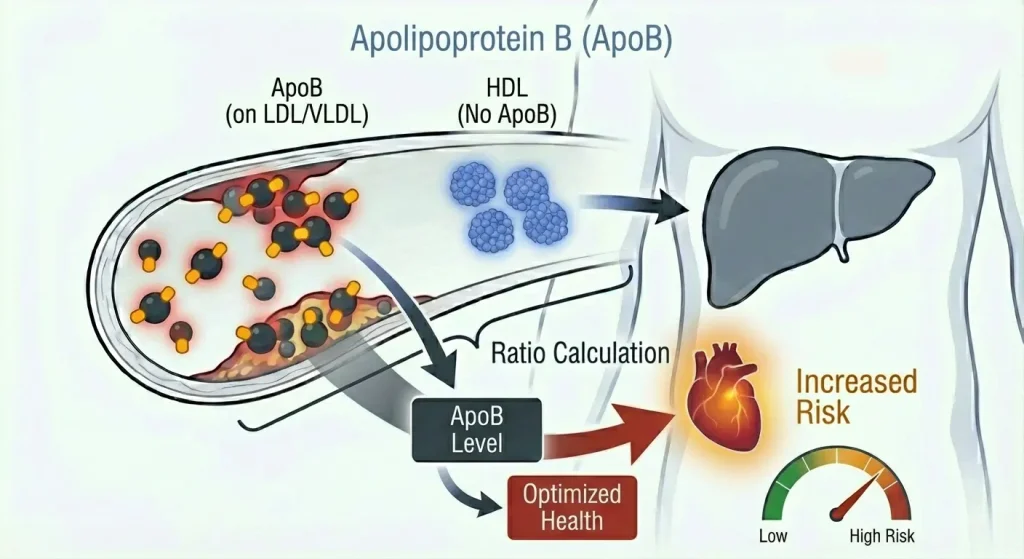
Apolipoprotein B (ApoB) is a protein that sits on the surface of atherogenic lipid particles. Every VLDL (very low-density lipoprotein), IDL (intermediate-density lipoprotein), and LDL (low-density lipoprotein) particle contains exactly one ApoB molecule.
This one-to-one relationship is what makes ApoB so powerful. By measuring ApoB, you’re directly counting the number of atherogenic particles circulating in your bloodstream. Each mg/dL of ApoB represents millions of particles capable of penetrating arterial walls and contributing to atherosclerosis.
Here’s why this matters: LDL cholesterol measures how much cholesterol is carried inside LDL particles. But the same amount of cholesterol can be packaged in many small particles or fewer large particles. Particle number drives cardiovascular risk far more than cholesterol content.
You could have 100 mg/dL of LDL cholesterol spread across many small particles (high ApoB, high risk) or concentrated in fewer large particles (lower ApoB, lower risk). Standard lipid panels measure cholesterol content and miss this critical distinction. ApoB reveals what’s actually happening.
VLDL particles are produced by the liver, carrying triglycerides to tissues. Each VLDL particle has one ApoB molecule. As VLDL releases triglycerides, it shrinks and becomes IDL, still carrying that one ApoB molecule. IDL further loses lipid content and becomes LDL, still with that same ApoB molecule. Eventually these particles are cleared from circulation by receptors that recognize ApoB.
When this system functions properly, particles deliver necessary lipids and get efficiently removed. Problems arise when particle production exceeds clearance, when particles become small and easily penetrate arterial walls, or when metabolic dysfunction creates a pro-atherogenic environment. ApoB tells you your total burden of these potentially dangerous particles.
Why ApoB Is Superior to LDL Cholesterol
The evidence supporting ApoB as a superior cardiovascular risk marker is overwhelming and comes from multiple lines of research.
Large epidemiological studies consistently show ApoB predicts cardiovascular events better than LDL cholesterol. The INTERHEART study examining heart attack risk across 52 countries found that ApoB and the ApoB/ApoA-I ratio were among the strongest predictors of myocardial infarction. The EPIC-Norfolk study, the Quebec Cardiovascular Study, and numerous others show similar results—when comparing ApoB and LDL cholesterol head-to-head, ApoB wins.
Discordance analysis reveals where LDL cholesterol fails. In approximately 20-30% of people, LDL cholesterol and ApoB tell different stories—one appears acceptable while the other is elevated. When this discordance occurs, ApoB consistently predicts cardiovascular events better than LDL cholesterol. Someone with “normal” LDL but elevated ApoB has higher risk than their LDL suggests. Someone with elevated LDL but normal ApoB has lower risk than their LDL suggests.
Mendelian randomization studies show that genetically determined ApoB levels causally drive atherosclerosis. People with genetic variants causing lifelong elevated ApoB have proportionally increased cardiovascular disease risk. This causal relationship is clear and consistent across populations.
Treatment trials demonstrate that cardiovascular benefit from statins, PCSK9 inhibitors, and other lipid-lowering medications correlates more closely with ApoB reduction than LDL cholesterol reduction. The magnitude of ApoB lowering predicts the magnitude of cardiovascular risk reduction across different interventions.
Why is ApoB superior? Because it measures what actually causes atherosclerosis—atherogenic particles penetrating arterial walls. LDL cholesterol is just a proxy that sometimes works and sometimes doesn’t. ApoB is the direct measurement.
The Science: How ApoB Drives Atherosclerosis
Understanding how atherogenic particles cause cardiovascular disease clarifies why counting particles matters more than measuring cholesterol content.
Atherosclerosis begins when ApoB-containing particles penetrate the arterial wall. The endothelium (arterial lining) normally acts as a barrier, but when damaged by hypertension, smoking, inflammation, or metabolic dysfunction, it becomes permeable. Small particles penetrate more easily than large particles, but all ApoB-containing particles can penetrate given sufficient time and exposure.
Once inside the arterial wall, trapped particles become oxidized. The subendothelial space contains reactive oxygen species and enzymes that modify lipoproteins. Oxidized LDL triggers inflammatory responses that drive plaque formation.
The immune system responds to these oxidized particles as foreign invaders. Macrophages infiltrate the arterial wall attempting to clear oxidized lipoproteins. They engulf particles and become “foam cells” filled with cholesterol. These foam cells form the core of atherosclerotic plaques.
Over time, plaques grow through continued particle infiltration, inflammatory responses, smooth muscle cell proliferation, and calcification. Eventually plaques can rupture, triggering blood clots that cause heart attacks and strokes.
The critical point: this entire process is driven by the number of atherogenic particles penetrating arterial walls, not by the amount of cholesterol they carry. More particles means more penetration, more oxidation, more inflammation, and more atherosclerosis. ApoB counts these particles. LDL cholesterol doesn’t.
The relationship between ApoB and cardiovascular risk is remarkably linear—the lower your ApoB, the lower your risk, with no apparent threshold where lowering further stops providing benefit. This suggests that particle burden itself is the driver, not some secondary factor correlated with cholesterol content.
Normal vs. Optimal ApoB Levels
Standard reference ranges vary slightly between laboratories but typically show:
Normal: Below 100 mg/dL
Borderline high: 100-129 mg/dL
High: 130 mg/dL and above
The problem with these ranges is they’re based on population averages that include metabolically unhealthy individuals with insulin resistance, obesity, and poor cardiovascular health. “Normal for the population” is not the same as “optimal for longevity and performance.”
Current evidence-based targets for ApoB:
For primary prevention (people without established cardiovascular disease): Below 90 mg/dL is reasonable, below 80 mg/dL is optimal. Many longevity-focused physicians target ApoB below 80 mg/dL or even lower for patients optimizing for maximum lifespan.
For secondary prevention (people with established cardiovascular disease, previous heart attack or stroke): Below 80 mg/dL minimum, ideally below 70 mg/dL or even lower depending on individual risk factors and treatment tolerance.
For people with very high genetic risk (familial hypercholesterolemia, strong family history of premature cardiovascular disease): Aggressive targets below 70 mg/dL, sometimes 60 mg/dL or lower.
Why such aggressive targets? Because the data shows that lower ApoB consistently correlates with lower cardiovascular events across populations. Unlike some biomarkers where extremely low levels raise concerns, the evidence for ApoB suggests that lower is better without an apparent floor.
Someone with ApoB at 95 mg/dL might be told they’re “normal.” But compared to someone with ApoB at 70 mg/dL, they have approximately 35% more atherogenic particles circulating, penetrating arterial walls, and contributing to plaque formation. Over decades, this difference matters enormously.
For high performers optimizing for longevity, target ApoB below 80 mg/dL. This requires comprehensive metabolic optimization and possibly medical intervention, but the cardiovascular risk reduction justifies the effort.
What Causes Elevated ApoB?
Understanding what drives high ApoB reveals what you need to optimize to lower it.
Genetic factors play a significant role in determining baseline ApoB levels. Familial hypercholesterolemia (FH) is a genetic condition affecting approximately 1 in 250 people, causing very high ApoB from birth due to defective LDL receptors that can’t efficiently clear particles from circulation. People with FH often have ApoB above 120-150 mg/dL despite lifestyle optimization and require aggressive medical treatment. More commonly, polygenic variants in genes affecting lipoprotein production, receptor function, and particle clearance create variation in how people respond to dietary factors and how efficiently they clear atherogenic particles.
Metabolic dysfunction and insulin resistance dramatically increase ApoB. Insulin resistance increases hepatic VLDL production—the liver overproduces triglyceride-rich particles that eventually become LDL. Insulin resistance also impairs LDL receptor activity, reducing particle clearance. The combination of increased production and decreased clearance substantially elevates ApoB. This is why insulin-resistant individuals often have elevated ApoB even when LDL cholesterol appears only moderately elevated—they’re producing many small, triglyceride-depleted particles.
Obesity and visceral fat drive ApoB elevation through multiple mechanisms. Visceral adiposity promotes insulin resistance, increases hepatic VLDL production through free fatty acid delivery to the liver, creates inflammatory cytokine production that impairs lipid metabolism, and reduces LDL receptor activity. Losing visceral fat is one of the most effective interventions for lowering ApoB in people with excess body fat.
Dietary factors influence ApoB, though effects vary between individuals. Excess saturated fat increases ApoB in many people, though responses are highly variable—some people are “hyper-responders” whose ApoB rises substantially, while others show minimal change. Trans fats from partially hydrogenated oils dramatically increase ApoB and should be completely eliminated. Excess refined carbohydrates and sugar don’t directly increase ApoB as much as they drive insulin resistance, which then increases ApoB through the mechanisms described above.
Thyroid function significantly impacts ApoB metabolism. Hypothyroidism reduces LDL receptor expression and activity, impairing particle clearance and causing ApoB to accumulate. Treating thyroid dysfunction often normalizes ApoB without additional intervention. Anyone with unexplained ApoB elevation should have comprehensive thyroid testing (TSH, free T4, free T3).
Physical inactivity impairs ApoB clearance. Regular exercise improves LDL receptor activity, enhances insulin sensitivity (reducing VLDL overproduction), and modestly lowers ApoB even when weight doesn’t change significantly.
Certain medications can elevate ApoB including corticosteroids, some immunosuppressants, anabolic steroids, and thiazide diuretics. If ApoB rises after starting a medication, discuss alternatives with your physician.
Age naturally increases ApoB as receptor function declines and metabolic efficiency decreases. This age-related increase is partly why cardiovascular disease risk increases with age, independent of other factors.
ApoB vs. LDL Cholesterol: Understanding Discordance
The 20-30% of people in whom ApoB and LDL cholesterol disagree represent one of the most important scenarios in cardiovascular risk assessment.
Concordance (ApoB and LDL agree) occurs in about 70% of people. High LDL and high ApoB together indicate elevated particle burden with elevated cholesterol content per particle—straightforward high risk requiring intervention. Low LDL and low ApoB together indicate favorable particle burden—lower risk.
Discordance Type 1 (Normal LDL, Elevated ApoB) occurs when you have many small particles carrying less cholesterol each. Your LDL cholesterol might be 110 mg/dL (acceptable), but your ApoB is 105 mg/dL (elevated). This means you have more atherogenic particles than your LDL suggests. This pattern typically occurs with insulin resistance, elevated triglycerides (above 150 mg/dL), low HDL (below 40-50 mg/dL), and metabolic dysfunction. Despite “normal” LDL, cardiovascular risk is substantially elevated because particle number drives atherosclerosis. This is the classic scenario where standard lipid panels give false reassurance while ApoB reveals true risk.
Discordance Type 2 (Elevated LDL, Normal ApoB) occurs when you have fewer large particles carrying more cholesterol each. Your LDL cholesterol might be 145 mg/dL (elevated), but your ApoB is 75 mg/dL (optimal). This means you have fewer atherogenic particles than your LDL suggests. This pattern typically occurs with good insulin sensitivity, low triglycerides (below 100 mg/dL), high HDL (above 60-70 mg/dL), and favorable metabolic health. Despite elevated LDL, cardiovascular risk is lower than standard assessment would suggest because you have fewer particles capable of penetrating arterial walls.
When discordance occurs, ApoB is the better predictor. Multiple studies show that people with normal LDL but elevated ApoB have higher cardiovascular event rates than people with elevated LDL but normal ApoB. Particle number wins over cholesterol content.
Clinical implications of discordance are profound. Someone with LDL at 110 mg/dL would typically receive no treatment based on standard guidelines. But if their ApoB is 110 mg/dL, they need intervention—likely metabolic optimization addressing insulin resistance, possibly medication if ApoB remains elevated. Conversely, someone with LDL at 150 mg/dL might reflexively receive a statin prescription. But if their ApoB is 75 mg/dL with excellent metabolic health, aggressive medication might not be necessary—continued monitoring and lifestyle optimization might be more appropriate.
This is precision medicine versus population-based algorithms. Measuring ApoB allows individualized risk assessment and treatment decisions rather than reflexive responses to LDL thresholds.
ApoB and Other Cardiovascular Risk Markers
ApoB provides the best assessment of atherogenic particle burden, but cardiovascular risk depends on multiple factors. Understanding how ApoB relates to other markers creates a complete risk picture.
ApoB and triglycerides are inversely related to particle size. High triglycerides (above 150 mg/dL) typically correlate with elevated ApoB and many small particles. Low triglycerides (below 100 mg/dL) typically correlate with lower or moderate ApoB and larger particles. When someone has elevated ApoB with high triglycerides, metabolic dysfunction is usually driving both—addressing insulin resistance often improves both markers simultaneously.
ApoB and HDL cholesterol often move in opposite directions. Metabolically healthy people typically have lower ApoB and higher HDL. Insulin-resistant individuals typically have higher ApoB and lower HDL. However, HDL is a marker of metabolic health, not a causal protective factor—raising HDL pharmacologically doesn’t reduce cardiovascular risk. The value in the relationship is that low HDL alongside high ApoB suggests metabolic dysfunction requiring comprehensive optimization.
ApoB and insulin resistance are strongly correlated. Fasting insulin above 5-7 μIU/mL typically correlates with elevated ApoB. As insulin resistance worsens, ApoB tends to rise because the liver overproduces VLDL particles and clearance mechanisms become impaired. Improving insulin sensitivity through weight loss, exercise, and metabolic optimization typically lowers ApoB substantially.
ApoB and inflammation (hs-CRP) independently contribute to cardiovascular risk. You can have low ApoB with high inflammation (elevated risk from inflammatory mechanisms) or high ApoB with low inflammation (elevated risk from particle burden). The combination of high ApoB and high hs-CRP represents particularly elevated risk because you have both high particle burden and an inflammatory environment that makes those particles more likely to penetrate arterial walls and become oxidized.
ApoB and blood pressure together determine arterial damage. Hypertension damages the endothelium, making it more permeable to atherogenic particles. High ApoB with high blood pressure accelerates atherosclerosis more than either factor alone. Controlling blood pressure reduces the rate at which particles penetrate arterial walls even when ApoB remains elevated.
ApoB and hemoglobin A1c reflect different aspects of metabolic health. Elevated A1c indicates poor glucose control and typically correlates with insulin resistance that drives high ApoB. But you can have elevated ApoB with normal A1c in early insulin resistance before glucose rises significantly—ApoB often deteriorates earlier than glucose markers. Both contribute independently to cardiovascular risk through different mechanisms.
How to Lower ApoB
Reducing ApoB requires addressing the factors that drive particle production and impair particle clearance.
Improve insulin sensitivity as the foundation of ApoB reduction. Lose excess body fat, particularly visceral fat, through sustained caloric deficit while maintaining muscle mass through resistance training. Exercise regularly with both aerobic training (improves insulin sensitivity directly) and resistance training (builds metabolically active muscle tissue). Reduce refined carbohydrates and added sugars that drive insulin resistance and hepatic VLDL overproduction. Optimize sleep—poor sleep dramatically worsens insulin sensitivity and increases ApoB. Manage chronic stress through stress reduction techniques, as elevated cortisol impairs insulin sensitivity.
Optimize dietary patterns to reduce particle production. Reduce saturated fat intake if you’re a hyper-responder (check ApoB response after dietary changes). Eliminate trans fats completely—they dramatically worsen ApoB. Increase soluble fiber from oats, beans, lentils, vegetables, and fruits—fiber binds cholesterol in the digestive tract and increases excretion, reducing particle production. Include plant sterols and stanols from fortified foods or supplements (2g daily can lower ApoB by 5-10%). Emphasize whole, unprocessed foods over refined and processed options. Some people benefit from increasing unsaturated fat (particularly monounsaturated fat from olive oil, avocados, nuts) while reducing saturated fat.
Address thyroid dysfunction if present. Hypothyroidism substantially elevates ApoB by reducing LDL receptor activity. Optimizing thyroid function (TSH, free T4, free T3) often normalizes ApoB without additional intervention. Always check thyroid function when ApoB is unexpectedly elevated.
Weight loss provides substantial ApoB reduction in people with excess body fat. Losing 10-20 pounds typically reduces ApoB by 10-20% or more, with greater reductions in people with significant visceral adiposity. The mechanism is primarily through improved insulin sensitivity and reduced hepatic VLDL production.
Exercise consistently for both immediate and long-term ApoB benefits. Aerobic exercise improves LDL receptor activity and insulin sensitivity. Resistance training builds muscle that improves glucose disposal and insulin function. Combined training typically reduces ApoB by 5-15% over 2-3 months even when weight loss is modest.
Consider medical interventions when lifestyle optimization isn’t sufficient. For people with ApoB above 100-120 mg/dL suggesting genetic factors like familial hypercholesterolemia, established cardiovascular disease, or high cardiovascular risk despite lifestyle optimization, medications have strong evidence supporting benefit. Statins lower ApoB by 20-55% depending on dose and type. PCSK9 inhibitors lower ApoB by 50-60% or more and are particularly effective for people who don’t tolerate statins or need additional reduction. Ezetimibe lowers ApoB by 15-20% by blocking cholesterol absorption. Bempedoic acid lowers ApoB by 15-25% and can be used when statins aren’t tolerated.
The decision to use medication should be based on ApoB level, comprehensive cardiovascular risk assessment including hs-CRP and insulin markers, presence of established cardiovascular disease or strong family history, response to lifestyle optimization, and individual tolerance for medication side effects.
ApoB and Metabolic Optimization Treatments
When elevated ApoB is driven by metabolic dysfunction—insulin resistance, visceral adiposity, and atherogenic particle overproduction—targeted interventions can support comprehensive metabolic improvement.
Metformin improves insulin sensitivity, which often substantially reduces ApoB even when LDL cholesterol doesn’t change dramatically. By improving metabolic health, metformin reduces hepatic VLDL overproduction and can lower ApoB by 5-15% in insulin-resistant individuals. This is particularly effective when insulin resistance is the primary driver of elevated ApoB.
GLP-1 medications (semaglutide, tirzepatide) produce significant weight loss and metabolic improvements that typically reduce ApoB by 10-20% or more. The mechanism is primarily through weight loss reducing visceral fat and improving insulin sensitivity, which decreases hepatic VLDL production. GLP-1s also have direct effects on lipid metabolism independent of weight loss. For people with elevated ApoB driven by obesity and insulin resistance, GLP-1s can be highly effective.
Hormone optimization may influence ApoB when hormonal imbalances contribute to metabolic dysfunction. Low testosterone in men is associated with higher ApoB, insulin resistance, and unfavorable body composition. Optimizing testosterone often improves ApoB alongside other metabolic benefits, though effects vary individually. In women, the hormonal changes of menopause typically increase ApoB substantially, and hormone optimization may provide benefits, though effects are variable and individualized.
These interventions work best as part of comprehensive metabolic optimization including nutrition, exercise, sleep, and stress management. The goal is addressing root causes of elevated ApoB—insulin resistance, visceral adiposity, and metabolic dysfunction—rather than just lowering a number in isolation.
ApoB in Different Populations
Understanding how ApoB behaves across different populations helps interpret individual results.
Young, metabolically healthy individuals typically have ApoB between 60-80 mg/dL. This reflects efficient particle clearance, low VLDL production, and favorable metabolic health. Young people with ApoB above 90-100 mg/dL likely have genetic factors affecting particle metabolism or early metabolic dysfunction requiring attention.
Insulin-resistant individuals typically have ApoB above 90-100 mg/dL even when LDL cholesterol appears only moderately elevated. The elevated ApoB reflects overproduction of small, triglyceride-depleted particles. This population benefits most from metabolic optimization addressing insulin resistance as the foundation of ApoB reduction.
People with familial hypercholesterolemia have ApoB above 120-150 mg/dL from birth due to genetic defects in LDL receptors. Despite optimal lifestyle, their ApoB remains dramatically elevated because they can’t efficiently clear particles. This population requires aggressive medical treatment—high-dose statins, PCSK9 inhibitors, or combination therapy—to achieve target ApoB levels below 80 mg/dL.
Athletes and highly active individuals sometimes show paradoxical patterns. Despite excellent metabolic health, some athletes have moderately elevated LDL and ApoB. The clinical significance is debated—some evidence suggests this occurs in the context of such favorable overall metabolic health (low inflammation, excellent insulin sensitivity, low triglycerides) that cardiovascular risk remains low. However, many longevity physicians still recommend targeting ApoB below 80 mg/dL even in metabolically healthy individuals.
Older adults typically have higher ApoB than younger people due to age-related decline in receptor function and metabolic efficiency. This partly explains why cardiovascular disease risk increases with age. However, healthy older individuals can still achieve ApoB below 80 mg/dL through lifestyle optimization and medical intervention when appropriate.
Women typically have lower ApoB than men at the same age before menopause due to protective effects of estrogen. After menopause, women’s ApoB increases substantially, often exceeding men’s levels. This dramatic increase explains much of the post-menopausal increase in cardiovascular disease risk.
Frequently Asked Questions
What is a good ApoB level?
For primary prevention (people without established cardiovascular disease), optimal is below 80 mg/dL, acceptable is below 90 mg/dL. For secondary prevention (people with established cardiovascular disease), target below 80 mg/dL minimum, ideally below 70 mg/dL. For people with genetic high risk, even more aggressive targets may be appropriate. The relationship between ApoB and cardiovascular risk is linear—lower is consistently better.
Is ApoB better than LDL cholesterol?
Yes. ApoB directly counts atherogenic particles while LDL cholesterol only measures cholesterol content. Studies consistently show ApoB predicts cardiovascular events better than LDL, especially in the 20-30% of people where the two markers are discordant. If you can only measure one lipid marker, measure ApoB. As Peter Attia emphasizes, ApoB is the gold standard for assessing atherogenic burden.
Can I have normal LDL but high ApoB?
Yes, and this occurs in approximately 10-15% of people. Normal LDL with elevated ApoB means you have many small particles carrying less cholesterol each. This pattern typically reflects insulin resistance, elevated triglycerides, and metabolic dysfunction. Despite “normal” LDL, your cardiovascular risk is elevated because particle number drives atherosclerosis. This is exactly why measuring ApoB matters—it reveals risk that standard lipid panels miss.
How quickly can I lower ApoB?
Dietary and lifestyle changes typically reduce ApoB by 5-20% within 4-8 weeks depending on baseline and adherence. Weight loss produces progressive reductions as you lose fat—expect 1-2% reduction per kilogram lost. Exercise shows benefits within 2-3 months of consistent training. Statins and other medications reduce ApoB within weeks—statins lower it by 20-55%, PCSK9 inhibitors by 50-60%. The timeline depends on baseline ApoB, underlying causes, and intervention intensity.
Why is my ApoB high when I eat healthy and exercise?
Several possibilities: genetic factors affecting particle production or clearance (familial hypercholesterolemia or polygenic variants), unrecognized insulin resistance or metabolic dysfunction despite healthy habits, thyroid dysfunction impairing particle clearance, or individual hyper-response to dietary saturated fat. Check fasting insulin, hemoglobin A1c, thyroid function (TSH, free T4, free T3), and consider genetic testing if ApoB remains above 100 mg/dL despite optimization.
Should I take a statin if my ApoB is elevated?
It depends on how elevated and your overall cardiovascular risk. ApoB above 100-120 mg/dL despite lifestyle optimization, particularly with established cardiovascular disease, strong family history, or elevated inflammation (high hs-CRP), warrants serious consideration of statin therapy. ApoB between 90-100 mg/dL might be addressed through continued lifestyle optimization if other risk factors are well-controlled. Below 90 mg/dL typically doesn’t require medication unless other high-risk features are present. Discuss comprehensive risk assessment with your physician.
Can ApoB be too low?
Unlike some biomarkers where extremely low levels raise concerns, the evidence for ApoB suggests lower is consistently better without an apparent floor. Some people naturally have ApoB in the 40-60 mg/dL range and remain healthy. The question is whether pharmacologically driving ApoB to extremely low levels (below 40-50 mg/dL) in people who don’t naturally have low ApoB creates problems. Current evidence doesn’t suggest major concerns, though very aggressive lipid lowering warrants monitoring for side effects.
Does ApoB replace the need for other lipid tests?
ApoB is the most important lipid marker, but comprehensive assessment still requires other markers. Triglycerides and HDL provide metabolic context. Hs-CRP assesses inflammation. Insulin and hemoglobin A1c evaluate insulin resistance. Lipoprotein(a) assesses genetic risk. The complete picture requires ApoB as the foundation plus markers that reveal the metabolic environment and additional risk factors.
Testing ApoB With ApexBlood
ApexBlood’s comprehensive blood panel includes apolipoprotein B (ApoB)—the single best marker for cardiovascular risk assessment that most standard panels don’t include.
Our testing also includes all markers necessary to understand your ApoB in complete context: LDL cholesterol, HDL cholesterol, triglycerides, VLDL cholesterol for lipid profile, cholesterol/HDL ratio and LDL/HDL ratio for metabolic context, high-sensitivity C-reactive protein (hs-CRP) for inflammation assessment, fasting insulin and hemoglobin A1c for insulin resistance evaluation, complete thyroid panel (TSH, free T4, free T3) for thyroid function affecting particle clearance, and complete blood count markers for overall health context.
This comprehensive approach reveals both your atherogenic particle burden (ApoB) and the metabolic factors driving it—insulin resistance, inflammation, thyroid function, and lipid metabolism patterns.
Most doctors don’t order ApoB because standard lipid panels don’t include it and many aren’t familiar with its superior predictive value. But the evidence is overwhelming—if you’re serious about understanding cardiovascular risk, ApoB is essential.
You can’t optimize what you don’t measure. Stop relying on incomplete lipid panels when ApoB reveals your true atherogenic burden.
Get comprehensive testing including ApoB – $189
The Bottom Line on ApoB
Apolipoprotein B is the single best lipid-related marker for cardiovascular risk assessment. It directly counts atherogenic particles—VLDL, IDL, and LDL—that penetrate arterial walls and cause atherosclerosis. LDL cholesterol is just a proxy that sometimes works and sometimes doesn’t.
The evidence is overwhelming: ApoB predicts cardiovascular events better than LDL cholesterol across multiple large studies. When ApoB and LDL disagree (which happens in 20-30% of people), ApoB is consistently the better predictor. The relationship between ApoB and cardiovascular risk is remarkably linear—lower ApoB means lower risk without an apparent threshold.
Optimal ApoB is below 80 mg/dL for people optimizing for longevity, below 90 mg/dL minimum for primary prevention, and below 80 mg/dL (ideally below 70 mg/dL) for secondary prevention. Standard “normal” ranges (below 100 mg/dL) are based on unhealthy populations and don’t represent optimal cardiovascular health.
Elevated ApoB is driven by genetic factors (familial hypercholesterolemia, polygenic variants), metabolic dysfunction (insulin resistance, visceral obesity), thyroid dysfunction, and lifestyle factors (diet, physical inactivity). Lowering ApoB requires addressing these root causes through metabolic optimization and medical intervention when necessary.
High performers don’t make cardiovascular risk decisions based on incomplete lipid panels that measure cholesterol content rather than particle number. They measure ApoB, understand their true atherogenic burden, and optimize accordingly.
As Peter Attia consistently emphasizes, if you can only measure one thing for cardiovascular risk assessment, measure ApoB. It’s the most accurate, most direct measurement of what actually drives atherosclerosis.
Stop accepting LDL cholesterol as adequate when ApoB reveals your true cardiovascular risk. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Apolipoprotein B levels and cardiovascular risk require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.