
Hematocrit: The Blood Viscosity Marker That Reveals Oxygen Capacity and Cardiovascular Risk
Your hemoglobin is 16.2 g/dL—excellent for oxygen-carrying capacity. But your hematocrit is 52%—meaning your blood is thicker than optimal, increasing cardiovascular risk and potentially impairing oxygen delivery despite high hemoglobin.
Or the opposite: your hemoglobin appears “normal” at 13.5 g/dL, but your hematocrit is 38%—confirming that your blood’s oxygen-carrying capacity is suboptimal and explaining why you feel chronically fatigued.
Hematocrit is the percentage of your blood volume occupied by red blood cells. It’s not just another number that moves with hemoglobin—it provides critical information about blood viscosity, hydration status, oxygen delivery efficiency, and cardiovascular risk that hemoglobin alone doesn’t reveal.
Too low, and you’re not delivering adequate oxygen to tissues. Too high, and your blood becomes viscous, flows sluggishly through small vessels, and increases risk of blood clots, stroke, and heart attack.
High performers don’t just optimize hemoglobin—they understand that hematocrit reveals whether that hemoglobin is packaged in a way that efficiently delivers oxygen without creating cardiovascular risk.
What Is Hematocrit?
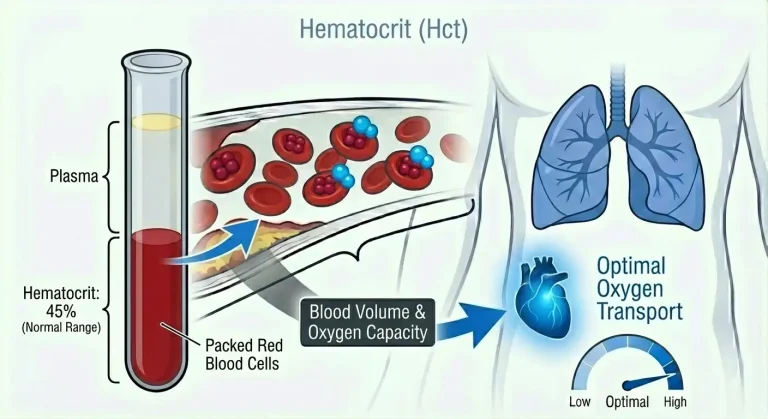
Hematocrit (abbreviated HCT or Hct) measures the percentage of total blood volume occupied by red blood cells. If your hematocrit is 45%, that means 45% of your blood volume consists of red blood cells, and 55% is plasma (the liquid component containing water, proteins, electrolytes, and other dissolved substances).
Hematocrit is determined by three factors: the number of red blood cells you have (RBC count), the size of those red blood cells (measured by MCV—mean corpuscular volume), and your plasma volume (affected by hydration status, blood volume regulation, and various physiological conditions).
The measurement process is straightforward. When blood is centrifuged (spun at high speed), red blood cells settle to the bottom due to their higher density, plasma rises to the top, and a thin layer of white blood cells and platelets (the “buffy coat”) sits between them. The percentage of the tube occupied by packed red blood cells is your hematocrit.
Modern automated analyzers calculate hematocrit from red blood cell count and mean cell volume rather than directly measuring it, but the principle remains the same—it tells you what fraction of your blood is cellular versus liquid.
Hematocrit and hemoglobin are closely related but provide different information. Hemoglobin measures the oxygen-carrying protein concentration in your blood. Hematocrit measures the percentage of blood that’s red blood cells. Both indicate oxygen-carrying capacity, but hematocrit also reveals blood viscosity and concentration, which directly impact cardiovascular function and oxygen delivery efficiency.
Why Hematocrit Matters for Performance and Health
Hematocrit determines blood viscosity—how thick or thin your blood is—which affects how easily it flows through vessels and delivers oxygen to tissues.
Optimal blood flow requires the right balance. Blood needs enough red blood cells to carry adequate oxygen, but not so many that it becomes thick and sluggish. When hematocrit rises too high (above 52-54% in men, above 46-48% in women), blood viscosity increases substantially. Thick blood flows more slowly through small capillaries, requires more force (higher blood pressure) to circulate, increases risk of blood clots forming, elevates stroke and heart attack risk, and can actually impair oxygen delivery to tissues despite high oxygen-carrying capacity.
This is the paradox of excessive hematocrit: you might have plenty of hemoglobin, but if blood is too viscous to flow efficiently through capillary beds, tissues don’t receive optimal oxygen. Elite athletes who use EPO or blood doping to increase hematocrit beyond 50-52% often experience diminishing returns or even performance decrements because blood viscosity impairs delivery.
Low hematocrit (below 38-40% in men, below 36-37% in women) indicates insufficient oxygen-carrying capacity. Your blood flows easily but doesn’t carry enough oxygen per unit volume. This causes reduced exercise capacity and endurance, chronic fatigue and low energy, impaired cognitive function and brain fog, cold intolerance, and prolonged recovery from physical exertion.
Oxygen delivery to tissues depends on the product of blood flow and oxygen content. Low hematocrit means low oxygen content per unit of blood. High hematocrit can impair blood flow. Optimal hematocrit balances these factors for maximum oxygen delivery.
Cardiovascular risk increases at both extremes. Very high hematocrit (above 54-55%) substantially increases blood clot risk, raises blood pressure through increased viscosity, elevates stroke and heart attack risk, and can trigger thrombotic events. Very low hematocrit indicates anemia requiring investigation of underlying causes, which might include nutrient deficiencies, bleeding, bone marrow disorders, or chronic disease.
Athletic performance requires hematocrit in the optimal range. Too low impairs oxygen delivery and limits aerobic capacity. Too high increases viscosity and cardiovascular strain. Elite endurance athletes typically maintain hematocrit at the higher end of normal ranges (48-50% for men, 42-46% for women) for maximum oxygen-carrying capacity without excessive viscosity. This is why professional cycling and other endurance sports strictly monitor and limit hematocrit—levels above 50% are often grounds for suspension due to presumed doping.
Normal vs. Optimal Hematocrit Levels
Standard reference ranges for hematocrit vary slightly by laboratory but typically show:
Men: 38.3-48.6% (some labs use 40-50%)
Women: 35.5-44.9% (some labs use 36-46%)
These ranges include sedentary, unhealthy populations and are designed to identify clinical anemia (too low) or polycythemia (too high) rather than optimal performance.
Optimal hematocrit for performance and health:
Men: 42-50%, ideally 44-48%
Women: 38-46%, ideally 40-44%
These targets provide excellent oxygen-carrying capacity without excessive blood viscosity. They reflect hematocrit levels seen in healthy, active individuals with good hydration and optimal red blood cell production.
Important considerations for interpretation:
Hydration status dramatically affects hematocrit. Dehydration concentrates blood, artificially elevating hematocrit by reducing plasma volume while red blood cell mass remains constant. Someone might have hematocrit at 50% when dehydrated but 46% when properly hydrated—same red blood cell mass, different plasma volume. This is why consistent hydration status matters for accurate hematocrit assessment.
Altitude and hypoxic exposure increase hematocrit. Living or training at altitude stimulates red blood cell production, raising hematocrit by 2-5% or more. This is a normal physiological adaptation to lower oxygen availability.
Testosterone and anabolic compounds increase hematocrit. Testosterone replacement therapy commonly raises hematocrit by 3-6% or more. Men on TRT require regular hematocrit monitoring. Modern TRT clinics generally consider hematocrit levels up to 54% acceptable for men on testosterone therapy, with intervention usually required if levels exceed this threshold.
Very high hematocrit (above 54-55% in men, above 48-50% in women) requires medical evaluation regardless of cause. Extremely elevated hematocrit creates significant cardiovascular risk.
Very low hematocrit (below 36-38% in men, below 33-35% in women) indicates anemia requiring investigation of underlying causes.
What Causes Low Hematocrit?
Low hematocrit and low hemoglobin typically occur together because both reflect reduced red blood cell mass or reduced hemoglobin content within cells. The causes are largely the same as those for low hemoglobin.
Iron deficiency is the most common cause globally. Inadequate dietary iron intake, poor iron absorption from gastrointestinal conditions, chronic blood loss from menstruation or GI bleeding, and increased iron demands during pregnancy or intense training all reduce iron availability. Without adequate iron, the body can’t produce enough hemoglobin or maintain optimal red blood cell production, lowering both hemoglobin and hematocrit.
Vitamin B12 and folate deficiencies impair red blood cell production in bone marrow. These vitamins are essential for DNA synthesis in rapidly dividing cells. Deficiency causes fewer red blood cells to be produced (lowering hematocrit) and the cells that are produced tend to be abnormally large (high MCV). B12 deficiency occurs from inadequate intake (strict vegan diets), poor absorption (pernicious anemia, gastric surgery, medications), or increased demands. Folate deficiency occurs from poor dietary intake or increased needs during pregnancy.
Chronic inflammation suppresses red blood cell production through inflammatory cytokines that impair iron utilization, reduce erythropoietin production, and shorten red blood cell lifespan. This creates “anemia of chronic disease” with low hemoglobin and hematocrit despite sometimes adequate iron stores. Common causes include autoimmune conditions, chronic infections, inflammatory bowel disease, and obesity-related inflammation.
Blood loss from any source reduces red blood cell mass and lowers hematocrit. Acute bleeding from trauma, surgery, or GI bleeding causes rapid hematocrit decline. Chronic bleeding from heavy menstruation, GI ulcers, or frequent blood donation gradually depletes red blood cells. After acute blood loss, hematocrit may initially appear normal (both red cells and plasma are lost proportionally) but drops as plasma volume is restored faster than red cell mass.
Bone marrow disorders impair red blood cell production including aplastic anemia, myelodysplastic syndromes, leukemia, or bone marrow suppression from chemotherapy or radiation.
Kidney disease reduces erythropoietin (EPO) production—the hormone that stimulates red blood cell production. Chronic kidney disease commonly causes anemia with low hematocrit.
Hemolysis (premature red blood cell destruction) lowers hematocrit through autoimmune destruction, genetic conditions like G6PD deficiency or sickle cell disease, mechanical destruction, or certain medications.
Overhydration or excessive plasma volume expansion can lower hematocrit without reducing absolute red blood cell mass. Pregnancy causes significant plasma volume expansion (up to 50%) that exceeds red blood cell mass increase, lowering hematocrit to 32-38% even in healthy pregnancies. This is “dilutional anemia”—not true anemia but rather dilution of red blood cells by expanded plasma volume.
What Causes High Hematocrit?
Elevated hematocrit occurs when red blood cell mass increases, plasma volume decreases, or both.
Dehydration is the most common cause of mildly elevated hematocrit. When you’re dehydrated, plasma volume contracts while red blood cell mass remains constant, concentrating red blood cells and artificially elevating hematocrit. Someone might have hematocrit at 51% when dehydrated but 47% when properly hydrated. This is why hydration status must be considered when interpreting hematocrit. Severe dehydration from illness, excessive sweating, inadequate fluid intake, or diuretic use can raise hematocrit substantially.
Chronic hypoxia (low oxygen) stimulates increased red blood cell production through elevated EPO. Living at high altitude naturally increases hematocrit by 3-6% or more as the body compensates for lower oxygen availability. Chronic lung disease (COPD, pulmonary fibrosis) causes chronically low blood oxygen, stimulating EPO and raising hematocrit. Sleep apnea creates intermittent hypoxia that can elevate hematocrit. Heavy smoking reduces oxygen delivery and impairs oxygen-carrying capacity, triggering compensatory red blood cell production.
Polycythemia vera is a bone marrow disorder causing uncontrolled red blood cell overproduction from a genetic mutation in blood-forming cells. Hematocrit progressively rises, often reaching 55-65% or higher if untreated. This substantially increases blood viscosity and elevates risk of blood clots, stroke, and heart attack. Polycythemia vera requires medical treatment including therapeutic phlebotomy and sometimes medications to suppress overproduction.
Testosterone therapy and anabolic steroid use stimulate red blood cell production. Testosterone commonly raises hematocrit by 3-8% or more depending on dose and individual response. While modest increases improve oxygen-carrying capacity and energy, levels above 54% typically warrant intervention. Men on testosterone replacement require regular hematocrit monitoring—when levels consistently exceed 54%, protocol adjustments are the standard approach to bring hematocrit back into acceptable ranges.
Secondary polycythemia from other causes includes kidney tumors or cysts producing excess EPO, other tumors producing EPO-like substances, and genetic conditions affecting oxygen sensing (Chuvash polycythemia and others).
Stress polycythemia (also called relative polycythemia or Gaisböck syndrome) occurs when plasma volume is chronically reduced without true increase in red blood cell mass. This is more common in men, particularly those who are hypertensive, overweight, and stressed. Hematocrit appears elevated (48-52%) but actual red blood cell mass is normal—the issue is reduced plasma volume.
Diuretic medications reduce plasma volume and can elevate hematocrit without increasing red blood cell mass.
Hematocrit and Related Blood Markers
Hematocrit exists within a system of related markers that provide complete context for red blood cell health and oxygen-carrying capacity.
Hemoglobin and hematocrit move together in predictable ways. A rough rule of thumb: hematocrit is approximately three times hemoglobin (if hemoglobin is 15 g/dL, hematocrit is typically around 45%). Significant deviation from this relationship suggests issues with red blood cell characteristics. If hematocrit is disproportionately high relative to hemoglobin, cells might be larger than normal or contain less hemoglobin per cell. If hematocrit is disproportionately low relative to hemoglobin, cells might be smaller or contain more hemoglobin per cell.
Red blood cell count (RBC) tells you how many red blood cells you have. Combined with hematocrit, this reveals average cell size. High hematocrit with normal RBC count suggests large cells (high MCV). High hematocrit with high RBC count suggests normal-sized or small cells.
MCV (mean corpuscular volume) measures average red blood cell size. Low MCV (below 80 fL) with normal-to-low hematocrit suggests iron deficiency or thalassemia—cells are smaller than normal. High MCV (above 100 fL) suggests B12 or folate deficiency, certain medications, or alcohol use—cells are larger than normal. Normal MCV with low hematocrit suggests anemia of chronic disease, recent blood loss, or mixed deficiencies.
MCH and MCHC measure hemoglobin content within red blood cells. These help classify anemia types and understand whether low hematocrit reflects too few cells, cells with inadequate hemoglobin, or both.
RDW (red cell distribution width) measures variation in red blood cell size. High RDW with abnormal hematocrit indicates significant variation in cell sizes, suggesting mixed nutritional deficiencies, recent blood loss with new cell production, or certain anemia types.
Platelet count can provide additional context. Very high hematocrit with high platelets might suggest polycythemia vera. Low hematocrit with abnormal platelets might suggest bone marrow disorders affecting multiple cell lines.
Hematocrit and Cardiovascular Risk
The relationship between hematocrit and cardiovascular risk follows a U-shaped curve—risk increases at both low and high extremes.
Low hematocrit increases cardiovascular risk through reduced oxygen delivery to cardiac muscle, requiring the heart to pump faster to deliver adequate oxygen (increased cardiac work), potential for increased heart failure risk in people with existing cardiac disease, and association with underlying conditions (chronic disease, nutritional deficiencies) that independently increase cardiovascular risk.
High hematocrit increases cardiovascular risk more dramatically through increased blood viscosity requiring higher blood pressure to circulate thick blood, dramatically elevated risk of blood clots (deep vein thrombosis, pulmonary embolism), increased stroke risk from both clots and impaired cerebral blood flow, elevated heart attack risk, and potential for microvascular complications as thick blood struggles to perfuse small vessels.
The risk from elevated hematocrit rises progressively above 50% and becomes substantial above 54-55% in men and 48-50% in women. Modern TRT clinics generally consider hematocrit levels up to 54% acceptable for men on testosterone therapy, with intervention usually required if levels exceed this threshold.
This is why testosterone therapy requires careful hematocrit monitoring. While optimizing testosterone provides numerous benefits, the hematocrit elevation it causes requires management through protocol adjustments when levels exceed acceptable ranges. Our standard approach is adjusting testosterone dosing, injection frequency, or other protocol modifications to maintain hematocrit at safe levels. Some physicians may recommend therapeutic phlebotomy (blood donation to reduce red blood cell mass), but this is not our preferred practice—we focus on protocol optimization to address elevated hematocrit at its source.
Similarly, athletes who artificially elevate hematocrit through EPO or blood doping face serious cardiovascular risks. Professional cyclists have died from blood clots and cardiac events related to excessive hematocrit elevation. This is why sports organizations strictly monitor and limit hematocrit—it’s not just about fair play, it’s about athlete safety.
How to Optimize Hematocrit
Optimizing hematocrit requires addressing the factors that affect red blood cell production and plasma volume.
For low hematocrit (below 40% in men, below 37% in women), the approach is similar to optimizing hemoglobin:
Ensure adequate iron intake and absorption through dietary sources (red meat, organ meats, shellfish) or supplementation if deficient. Check ferritin—target 50-100 ng/mL or higher for optimal red blood cell production.
Optimize vitamin B12 (target above 400-500 pg/mL) and folate through diet or supplementation, particularly important for vegans, vegetarians, and people with absorption issues.
Consume adequate protein for red blood cell production—at least 0.8-1.0 g/kg body weight, more for athletes.
Address any chronic blood loss including heavy menstruation requiring gynecological evaluation, gastrointestinal bleeding requiring investigation, or excessive blood donation (limit to 2-3 times yearly if struggling to maintain hematocrit).
Reduce chronic inflammation if present through addressing underlying inflammatory conditions, weight loss if obese, and dietary optimization. Check hs-CRP to assess inflammation.
Investigate underlying medical conditions if hematocrit remains low despite nutritional optimization—kidney disease, bone marrow disorders, or other causes require medical management.
For high hematocrit (above 50% in men, above 46% in women), the approach depends on the cause:
Ensure adequate hydration. Drink enough water daily to maintain proper plasma volume. Chronic mild dehydration is common and artificially elevates hematocrit.
If on testosterone therapy and hematocrit exceeds 54%, discuss protocol adjustments with your physician. Our standard approach focuses on modifying the protocol to address elevated hematocrit—this might include reducing testosterone dose, increasing injection frequency to create more stable levels with lower peaks, or other protocol modifications that bring hematocrit back into acceptable ranges. Some physicians may recommend therapeutic phlebotomy (donating blood to reduce red blood cell mass), though this is not our preferred practice. Always follow your personal physician’s recommendations, as individual circumstances vary.
If living at altitude or recently returned from altitude, understand this is a normal adaptation. Hematocrit gradually declines over weeks to months after returning to sea level.
Avoid dehydration, particularly if using diuretics, exercising heavily, or living in hot climates.
If hematocrit is above 54-55% without testosterone therapy or other obvious cause, seek medical evaluation for polycythemia vera or other causes of pathological red blood cell overproduction.
Hematocrit in Athletes and Active Individuals
Athletes pay close attention to hematocrit because it directly impacts oxygen delivery and performance while also indicating potential health risks.
Endurance athletes typically maintain hematocrit at the higher end of normal ranges. Male endurance athletes often have hematocrit around 44-48%, female endurance athletes around 40-44%. This reflects training adaptations, optimal nutrition, and sometimes altitude training effects.
The performance benefits of higher hematocrit are real but have limits. Increasing hematocrit from 42% to 47% improves oxygen-carrying capacity and typically enhances endurance performance. But increasing from 47% to 52% provides diminishing returns as blood viscosity begins to impair flow through capillaries. Above 52%, performance often declines despite higher oxygen-carrying capacity because blood is too thick to deliver oxygen efficiently.
This is why EPO doping targets specific hematocrit levels (typically 48-50%) rather than pushing as high as possible. Dopers understand that excessive hematocrit impairs performance and increases death risk.
Professional cycling banned EPO in the 1990s partly due to mysterious deaths of young, healthy cyclists from cardiac events and blood clots—all had elevated hematocrit from EPO use. The sport now maintains a “health threshold” of 50% hematocrit—athletes above this level are suspended until hematocrit normalizes, regardless of whether doping is proven.
For natural athletes optimizing performance:
Focus on maintaining hematocrit in the 44-48% range for men, 40-44% range for women through optimal nutrition, adequate iron and B12 status, appropriate training volume and recovery, and altitude training if accessible.
Monitor hematocrit regularly, particularly if using altitude training or hypoxic devices that stimulate red blood cell production.
Maintain excellent hydration—chronic dehydration artificially elevates hematocrit and impairs performance through reduced blood volume.
If hematocrit approaches or exceeds 50% (men) or 46% (women), evaluate hydration status, consider whether altitude exposure is creating excessive elevation, and consult with a sports medicine physician about cardiovascular risk.
Frequently Asked Questions
What is a good hematocrit level?
For men, optimal is 42-50%, ideally 44-48%. For women, optimal is 38-46%, ideally 40-44%. These levels provide excellent oxygen-carrying capacity without excessive blood viscosity. Standard “normal” ranges are wider but optimal performance requires staying in the middle-to-upper portion of normal ranges.
What does it mean if hematocrit is high but hemoglobin is normal?
This is unusual and suggests either laboratory error, significant red blood cell size variation (measured MCV might not reflect true average), dehydration affecting hematocrit more than hemoglobin measurement, or in rare cases, technical issues with the blood sample. Hematocrit and hemoglobin typically move together proportionally. Repeat testing when well-hydrated to clarify.
Can dehydration cause high hematocrit?
Yes, absolutely. Dehydration is one of the most common causes of mildly elevated hematocrit. When plasma volume contracts due to inadequate fluid intake, sweating, or diuretic use, red blood cells become concentrated and hematocrit rises. Someone might have hematocrit at 51% when dehydrated but 46% when properly hydrated. Always consider hydration status when interpreting hematocrit.
Is hematocrit of 50% dangerous?
It depends on context and individual factors. For men, 50% is at the upper limit of normal and not necessarily dangerous, particularly if well-hydrated and without cardiovascular risk factors. But it warrants monitoring and investigation of causes—dehydration, testosterone use, altitude exposure, or other factors. Modern TRT clinics generally consider levels up to 54% acceptable for men on testosterone therapy. For women, 50% is significantly elevated and requires medical evaluation.
Does testosterone always increase hematocrit?
Testosterone therapy increases hematocrit in most men, though the magnitude varies. Typical increase is 3-8% or more. Some men experience larger increases requiring protocol adjustments when hematocrit exceeds 54%. Regular hematocrit monitoring (every 3-6 months) is essential for men on testosterone replacement. Our standard approach to elevated hematocrit on TRT is adjusting the protocol—modifying dose, injection frequency, or other factors—rather than therapeutic phlebotomy.
What should I do if my hematocrit is high on testosterone therapy?
If your hematocrit exceeds 54% on testosterone therapy, discuss protocol adjustments with your physician. Standard approaches include reducing testosterone dose, increasing injection frequency to lower peak levels, or other protocol modifications to bring hematocrit into acceptable ranges. Some physicians may recommend therapeutic phlebotomy (blood donation), though this is not universally preferred as a long-term management strategy. Always follow your personal physician’s recommendations, as individual circumstances and medical opinions vary. The goal is maintaining hematocrit at safe levels while preserving testosterone’s benefits.
Can you have normal hematocrit but low hemoglobin?
This is unusual. Hematocrit and hemoglobin typically move together proportionally. If hematocrit appears normal but hemoglobin is low, possible explanations include significant red blood cell size variation (high MCV with fewer but larger cells), laboratory error or technical issues, or plasma protein abnormalities affecting measurements. Repeat testing and checking MCV will clarify.
Does altitude training increase hematocrit permanently?
Altitude exposure increases hematocrit by 2-5% or more as the body adapts to lower oxygen availability. This adaptation takes 2-4 weeks to develop fully. After returning to sea level, hematocrit gradually declines over several weeks to months as the body no longer needs elevated red blood cell mass for adequate oxygenation. The increase is not permanent but can provide temporary performance benefits during the decline period.
Testing Hematocrit With ApexBlood
ApexBlood’s comprehensive blood panel includes hematocrit as part of the complete blood count (CBC), along with all related markers necessary to understand your oxygen-carrying capacity, blood viscosity, and red blood cell health: hemoglobin for oxygen-carrying protein, RBC count for number of red blood cells, MCV (mean corpuscular volume) for red blood cell size, MCH and MCHC for hemoglobin content within cells, and RDW for variation in red blood cell size.
Our testing also includes critical markers that reveal what’s driving your hematocrit levels: ferritin for iron storage, iron and TIBC for current iron status, vitamin B12 for red blood cell production, and complete metabolic markers to assess overall health.
This comprehensive approach reveals not just your hematocrit level but the complete picture—whether elevated hematocrit reflects true red blood cell increase or dehydration, whether low hematocrit is from iron deficiency, B12 deficiency, or chronic disease, and whether your hematocrit represents optimal oxygen-carrying capacity or cardiovascular risk.
Understanding hematocrit requires context from multiple markers. You need to know if the ratio of hematocrit to hemoglobin is normal, whether red blood cells are the right size, whether iron stores support optimal production, and whether you’re maintaining the right balance between oxygen-carrying capacity and blood viscosity.
You can’t optimize what you don’t measure. Stop accepting hematocrit results without understanding what they mean for oxygen delivery, blood viscosity, and cardiovascular health.
Get comprehensive testing including hematocrit and complete blood count – $189
The Bottom Line on Hematocrit
Hematocrit measures the percentage of blood volume occupied by red blood cells and reveals critical information about oxygen-carrying capacity, blood viscosity, and cardiovascular risk that hemoglobin alone doesn’t provide.
Optimal hematocrit for men is 42-50%, ideally 44-48%. For women, optimal is 38-46%, ideally 40-44%. These levels balance excellent oxygen delivery with safe blood viscosity. Too low impairs oxygen transport and causes fatigue. Too high increases blood viscosity and cardiovascular risk.
Hematocrit and hemoglobin typically move together proportionally. Low hematocrit usually indicates the same conditions as low hemoglobin—iron deficiency, B12 or folate deficiency, chronic disease, or blood loss. High hematocrit indicates dehydration, chronic hypoxia, polycythemia, or medication effects (particularly testosterone).
The most common cause of mildly elevated hematocrit is dehydration—always consider hydration status when interpreting results. For men on testosterone therapy, modern TRT clinics generally consider hematocrit levels up to 54% acceptable, with protocol adjustments recommended when levels exceed this threshold. Our standard approach focuses on modifying testosterone protocols rather than therapeutic phlebotomy, though individual physicians may have different recommendations based on specific circumstances.
High performers understand that optimal oxygen delivery requires the right balance—enough red blood cells to carry oxygen efficiently, but not so many that blood becomes thick and flow is impaired. Hematocrit reveals whether you’ve achieved that balance.
Stop accepting hematocrit results without understanding what they mean for performance and cardiovascular health. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Hematocrit levels and red blood cell health require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.