
Neutrophils: The Frontline Immune Cells That Reveal Infection, Inflammation, and Hidden Immune Dysfunction
Your white blood cell count is 7,500/μL—perfectly normal. Your doctor says your immune system looks fine. But buried in the differential, your neutrophils are 2,800/μL—below the normal range of 1,500-7,800/μL, technically within some lab ranges but at the absolute lower limit.
Nobody mentions it because the total WBC count appears “normal.” Meanwhile, your neutrophil percentage is 37%—well below the optimal 40-70%. Your body’s primary bacterial defense system is compromised, leaving you vulnerable to infections that your immune system should easily handle.
Or the opposite: your neutrophils are 6,200/μL with a percentage of 82%—technically within some reference ranges but dramatically elevated, indicating chronic inflammation, ongoing infection, or stress response that’s overwhelming your immune system.
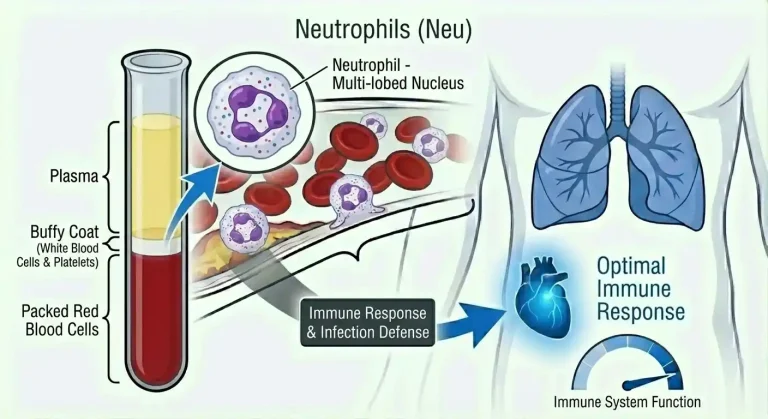
Neutrophils are your body’s rapid-response infection fighters—the first immune cells to arrive at infection sites, the primary defense against bacterial and fungal infections, and sensitive markers of inflammation, stress, and bone marrow function. Changes in neutrophil count and percentage reveal infections before you feel sick, chronic inflammatory states accelerating aging and disease, bone marrow dysfunction or medication side effects, and stress, metabolic dysfunction, or autoimmune processes.
High performers don’t just check total white blood cell count—they understand that neutrophil count and percentage provide critical information about immune function, inflammatory burden, and infection risk that total WBC misses.
What Are Neutrophils?
Neutrophils are the most abundant type of white blood cell in most people, typically comprising 40-70% of total white blood cells. They’re a type of granulocyte—white blood cells containing granules filled with antimicrobial proteins and enzymes.
Normal neutrophil count (absolute neutrophil count or ANC) ranges from approximately 1,500-7,800 cells/μL (some labs use 1,800-7,700/μL). In healthy adults, neutrophils typically number 2,500-6,000/μL.
Neutrophils are produced in bone marrow from stem cells. Production takes about 10-14 days from stem cell to mature neutrophil. The bone marrow maintains a large reserve of mature neutrophils that can be rapidly released into circulation when needed—this is why neutrophil count can increase dramatically within hours of infection or inflammation.
Neutrophils circulate in blood for only 6-8 hours before migrating into tissues where they live for 1-2 days before dying. This short lifespan means neutrophil populations turn over rapidly, making neutrophil count a sensitive marker of acute changes in immune status, bone marrow function, and infection/inflammation.
The primary function of neutrophils is defending against bacterial and fungal infections through several mechanisms. When infection or tissue damage occurs, neutrophils are the first immune cells to arrive—typically within minutes to hours. They migrate from blood vessels into infected tissues following chemical signals (chemotaxis). Once at the infection site, neutrophils engulf and destroy bacteria and fungi through phagocytosis (literally “cell eating”), release antimicrobial proteins and enzymes from their granules that kill pathogens, form neutrophil extracellular traps (NETs)—web-like structures of DNA and antimicrobial proteins that trap and kill pathogens, and produce reactive oxygen species that kill microorganisms.
Neutrophils are essentially suicide bombers of the immune system. They arrive at infection sites, kill pathogens aggressively, and die in the process. Dead neutrophils are a major component of pus. The body must constantly produce new neutrophils to replace those dying in the course of normal immune surveillance and infection fighting.
Beyond fighting infection, neutrophils participate in inflammatory responses, interact with other immune cells to coordinate immune responses, release chemical signals (cytokines) that recruit additional immune cells, and contribute to tissue damage in some autoimmune and inflammatory conditions when their powerful antimicrobial mechanisms are misdirected against the body’s own tissues.
Why Neutrophil Count Matters for Health and Performance
Neutrophil count directly determines your ability to fight bacterial and fungal infections and reveals important information about immune function, inflammation, bone marrow health, and overall physiological status.
Infection risk depends critically on neutrophil count. Normal counts (2,500-7,000/μL) provide excellent bacterial and fungal defense. You can fight off most infections effectively. Mild neutropenia (1,000-1,500/μL) increases infection risk modestly. You’re more susceptible to bacterial and fungal infections, particularly if exposed to high pathogen loads or have other immune compromises. Moderate neutropenia (500-1,000/μL) substantially increases infection risk. Bacterial infections that would be minor in healthy people can become serious. Dental procedures, minor cuts, and normal bacterial exposures pose greater risk. Severe neutropenia (below 500/μL) creates critical infection risk. Even normal gut bacteria can cause life-threatening infections. This level requires medical monitoring and often preventive antibiotics.
People with chronically low neutrophils (even in the 1,500-2,500/μL range) often notice they get sick more frequently, take longer to recover from infections, develop infections from minor injuries or dental work, and experience recurrent skin infections, sinusitis, or other bacterial problems.
Athletic performance and recovery depend partly on immune function. Low neutrophils impair recovery from intense training—exercise creates muscle damage and inflammation that requires immune cell participation for repair. Increase vulnerability to infections during heavy training periods when immune system is stressed. Create longer recovery times and increased injury risk. Athletes with chronically suppressed neutrophils often struggle with frequent illness interrupting training cycles.
Chronic inflammation is reflected in neutrophil elevation. Persistently elevated neutrophils (above 6,000-7,000/μL without acute infection) indicate chronic inflammatory state, ongoing tissue damage or infection, metabolic dysfunction (obesity, insulin resistance produce chronic inflammation), cardiovascular disease (atherosclerosis is inflammatory), and autoimmune conditions or other chronic diseases. This chronic elevation accelerates aging, increases cardiovascular risk, and contributes to multiple chronic diseases.
Stress response dramatically affects neutrophils. Acute physical or psychological stress causes rapid neutrophil elevation through cortisol and adrenaline release. This is why neutrophils can spike to 10,000-15,000/μL during intense exercise, after surgery or trauma, or during extreme psychological stress. Chronic stress can maintain moderately elevated neutrophils (6,000-8,000/μL), contributing to inflammatory burden.
Bone marrow health is revealed through neutrophil production. Declining neutrophils can be an early sign of bone marrow suppression from medications (particularly chemotherapy, certain antibiotics, anti-inflammatory drugs), bone marrow failure or infiltration, nutritional deficiencies affecting production (vitamin B12, folate, copper), or autoimmune destruction of neutrophils or bone marrow cells.
Normal vs. Optimal Neutrophil Count
Standard reference ranges for absolute neutrophil count (ANC) vary by laboratory but typically show:
Normal: 1,500-7,800 cells/μL (some labs use 1,800-7,700/μL or 2,000-7,500/μL)
Neutrophil percentage of total white blood cells: 40-70% (some labs use 45-75%)
These ranges include many people with suboptimal immune function, chronic inflammation, or stress responses. “Normal for the population” isn’t the same as “optimal for infection defense and minimal inflammatory burden.”
Optimal neutrophil count for health and performance:
Absolute neutrophil count: 2,500-6,000/μL, ideally 3,000-5,000/μL
Neutrophil percentage: 45-65%, ideally 50-60%
These targets provide excellent bacterial and fungal defense without excessive inflammatory activity. They reflect neutrophil levels seen in healthy, non-stressed individuals with good immune function and minimal chronic inflammation.
Important considerations for interpretation:
Neutrophils naturally vary throughout the day and in response to various stimuli. Count can increase by 2,000-3,000/μL or more with exercise, stress, meals, or other acute stimuli. This is why consistent testing conditions matter—ideally fasting, morning draws, when not acutely stressed.
Ethnic variation exists in baseline neutrophil counts. People of African, Middle Eastern, and some other ancestries often have baseline neutrophil counts of 1,200-2,500/μL—lower than typical reference ranges but normal for them. This is called benign ethnic neutropenia and doesn’t increase infection risk. What matters is the individual’s baseline pattern, not comparison to population averages.
Age affects neutrophil counts. Newborns have high neutrophils that decline in the first few days of life. Children often have lower neutrophil counts than adults. Older adults may have slightly lower baseline counts due to declining bone marrow reserve.
Neutrophil percentage relative to total WBC matters as much as absolute count. If total WBC is normal but neutrophils are low (below 40%), this indicates neutropenia even if absolute count appears borderline normal. Conversely, if total WBC is elevated and neutrophils make up 75-85% of the total, this indicates significant neutrophil-predominant inflammation or infection.
Very high neutrophil counts (above 10,000-12,000/μL) without acute infection or stress require investigation for chronic inflammatory conditions, undiagnosed infections, bone marrow disorders, or malignancies.
Very low neutrophil counts (below 1,500/μL) always require investigation to identify the cause and assess infection risk.
What Causes Low Neutrophils (Neutropenia)?
Neutropenia results from decreased production, increased destruction, or redistribution of neutrophils from circulation into tissues or marginal pools.
Decreased neutrophil production occurs when bone marrow can’t produce adequate neutrophils.
Medications are the most common cause of acquired neutropenia. Chemotherapy drugs directly suppress bone marrow and cause predictable neutropenia—counts typically drop 7-14 days after treatment and recover 14-21 days post-treatment. Certain antibiotics particularly cause neutropenia including sulfa drugs (trimethoprim-sulfamethoxazole), vancomycin, beta-lactams (penicillins, cephalosporins) in some people, and others. Anti-inflammatory medications including NSAIDs, certain disease-modifying antirheumatic drugs (methotrexate, sulfasalazine), and others. Antithyroid medications (methimazole, propylthiouracil) commonly cause neutropenia requiring monitoring. Anticonvulsants (valproic acid, carbamazepine, phenytoin) can suppress bone marrow. Antipsychotics, particularly clozapine, carry significant neutropenia risk requiring regular monitoring.
Nutritional deficiencies affecting bone marrow production include vitamin B12 deficiency (impairs DNA synthesis in rapidly dividing cells like neutrophil precursors), folate deficiency (same mechanism as B12), copper deficiency (rare but causes neutropenia and anemia), and severe protein-calorie malnutrition affecting all blood cell production.
Bone marrow disorders impair neutrophil production including aplastic anemia (bone marrow failure affecting all cell lines), myelodysplastic syndromes (abnormal stem cells producing ineffective blood cells), leukemia (cancerous cells crowding out normal production), bone marrow infiltration by lymphoma or metastatic cancer, and myelofibrosis (scarring of bone marrow impairing production).
Viral infections commonly cause temporary neutropenia. Many viruses including influenza, Epstein-Barr virus (mono), cytomegalovirus, HIV, hepatitis viruses, and COVID-19 can suppress bone marrow production or increase neutrophil destruction. Neutropenia typically resolves as viral infection clears but can persist with chronic viral infections like HIV.
Increased neutrophil destruction occurs when neutrophils are removed from circulation faster than bone marrow can replace them.
Autoimmune neutropenia develops when the immune system produces antibodies against neutrophils, marking them for destruction. This can be primary (isolated neutropenia) or occur as part of broader autoimmune conditions like systemic lupus erythematosus (SLE), rheumatoid arthritis (particularly Felty’s syndrome—RA with splenomegaly and neutropenia), or other autoimmune diseases.
Drug-induced immune neutropenia occurs when medications trigger antibody formation against neutrophils. This differs from direct bone marrow suppression—the bone marrow produces neutrophils normally but antibodies cause rapid destruction. Many medications can trigger this including certain antibiotics, quinine, and others.
Hypersplenism—an enlarged spleen—sequesters and destroys neutrophils (along with other blood cells). Causes of splenomegaly include liver disease with portal hypertension (cirrhosis), blood disorders, infections (particularly chronic malaria in endemic areas), and lymphomas.
Sepsis and overwhelming infection can consume neutrophils faster than production. Severe bacterial infections cause neutrophils to migrate into tissues in massive numbers and die fighting infection, potentially depleting circulating counts even as bone marrow tries to compensate.
Benign ethnic neutropenia is common in people of African, Middle Eastern, West Indian, and some other ancestries. Baseline neutrophil counts are typically 1,000-2,500/μL—lower than standard reference ranges but completely normal for these individuals. This doesn’t increase infection risk, doesn’t require treatment, and persists lifelong. It’s important to recognize this pattern to avoid unnecessary workups and interventions.
Congenital neutropenias are rare genetic conditions causing lifelong low neutrophils including cyclic neutropenia (neutrophil count cycles regularly, typically every 21 days from normal to very low), severe congenital neutropenia (Kostmann syndrome—very low counts from birth), and other inherited bone marrow failure syndromes.
What Causes High Neutrophils (Neutrophilia)?
Neutrophilia (elevated neutrophil count above 7,000-8,000/μL) results from increased production, mobilization of bone marrow reserves, or stress-induced release.
Infection is the most common cause of neutrophilia. Bacterial infections typically cause pronounced neutrophil elevation (10,000-20,000/μL or higher) as the bone marrow responds to infection by releasing reserves and increasing production. Common bacterial infections include pneumonia, urinary tract infections, skin and soft tissue infections (cellulitis, abscesses), appendicitis and other intra-abdominal infections, and meningitis. The degree of neutrophilia often correlates with infection severity. Fungal infections also stimulate neutrophil production and release.
Note: Viral infections typically don’t cause neutrophilia—they usually cause lymphocyte elevation with normal or low neutrophils. Neutrophilia with infection suggests bacterial rather than viral cause.
Inflammation from non-infectious causes stimulates neutrophil production and release. Inflammatory conditions causing neutrophilia include rheumatoid arthritis and other autoimmune diseases, inflammatory bowel disease (Crohn’s disease, ulcerative colitis), vasculitis, tissue damage from trauma, surgery, burns, or myocardial infarction (heart attack), gout and other crystal arthropathies during acute flares, and acute pancreatitis.
Stress response causes rapid neutrophil elevation through cortisol and adrenaline effects. Physical stress from intense exercise, surgery or trauma, acute illness or pain, severe burns, or seizures. Psychological stress from extreme anxiety, panic attacks, or acute psychological trauma. Metabolic stress from diabetic ketoacidosis, hyperthyroidism, or acute metabolic derangements. These stress-induced elevations are typically temporary, resolving hours to days after the stressor resolves.
Medications can increase neutrophil counts. Corticosteroids (prednisone, dexamethasone, others) reliably increase neutrophils by mobilizing bone marrow reserves and reducing migration into tissues—neutrophils can rise to 10,000-20,000/μL or higher with high-dose steroids. Lithium stimulates neutrophil production and commonly elevates counts. Epinephrine and other catecholamines cause acute neutrophil release. G-CSF (granulocyte colony-stimulating factor) and GM-CSF used to treat neutropenia dramatically increase neutrophil production.
Smoking elevates neutrophil counts chronically. Smokers typically have neutrophil counts 1,000-3,000/μL higher than non-smokers due to chronic inflammatory stimulation. Counts gradually normalize after smoking cessation.
Obesity and metabolic syndrome cause chronic mild neutrophilia through chronic low-grade inflammation. Visceral adipose tissue produces inflammatory cytokines that stimulate neutrophil production. Insulin resistance and metabolic dysfunction contribute to inflammatory state. People with obesity often have neutrophil counts of 5,000-8,000/μL reflecting chronic inflammatory burden.
Pregnancy increases neutrophil counts, particularly in the third trimester. Counts of 8,000-12,000/μL are normal during pregnancy and return to baseline postpartum.
Bone marrow disorders can cause primary neutrophilia where the bone marrow overproduces neutrophils independent of normal regulatory signals. Chronic myeloid leukemia (CML) causes very high neutrophil counts (often 15,000-100,000/μL or more) along with immature white blood cells in circulation. Polycythemia vera commonly causes mild neutrophilia alongside elevated red blood cells and platelets. Essential thrombocythemia and primary myelofibrosis can cause neutrophilia. Leukemoid reaction—extreme neutrophilia (above 50,000/μL) that mimics leukemia but is reactive to severe infection, inflammation, or malignancy rather than due to blood cancer itself.
Malignancy can cause neutrophilia through several mechanisms. Tumors producing G-CSF or other growth factors stimulate neutrophil production (paraneoplastic neutrophilia). Tumor necrosis and inflammation stimulate neutrophil release. Bone marrow metastases can disrupt normal regulation.
Post-splenectomy commonly causes mild chronic neutrophilia because the spleen normally removes some neutrophils from circulation. After splenectomy, counts typically increase by 1,000-2,000/μL and may remain mildly elevated indefinitely.
Understanding Neutrophil Percentage vs. Absolute Count
Both neutrophil percentage (portion of total WBC that’s neutrophils) and absolute neutrophil count (actual number of neutrophils per microliter) provide important information, but they tell different stories.
Absolute neutrophil count (ANC) is calculated by multiplying total WBC by neutrophil percentage. For example, total WBC 6,000/μL × 60% neutrophils = 3,600/μL absolute neutrophil count. ANC tells you the actual number of infection-fighting neutrophils you have circulating. This is what determines infection-fighting capacity.
Neutrophil percentage tells you the proportion of your white blood cells that are neutrophils versus other types (lymphocytes, monocytes, eosinophils, basophils). Changes in percentage can occur even when absolute count remains normal.
High neutrophil percentage with normal absolute count (neutrophil-predominant pattern) suggests relative increase in neutrophils compared to other white blood cells. This occurs with stress responses that increase neutrophils while suppressing lymphocytes, chronic inflammation causing neutrophil predominance, or viral infections that decrease lymphocytes (causing relative neutrophil increase even when absolute neutrophil count is normal).
Low neutrophil percentage with normal absolute count (lymphocyte-predominant pattern) suggests relative increase in lymphocytes compared to neutrophils. This is common in viral infections (lymphocytes increase to fight virus while neutrophils remain normal), chronic lymphocytic leukemia (lymphocytes massively increase), or after viral illness recovery (lymphocytes elevated during recovery phase).
Both high (neutrophilia with high percentage above 75-80%) indicates bacterial infection, severe inflammation, or bone marrow disorder producing excess neutrophils. Total WBC and neutrophil count are both elevated.
Both low (neutropenia with low percentage below 40%) indicates bone marrow suppression, autoimmune destruction, or other processes specifically affecting neutrophil production or survival. This is true neutropenia requiring investigation.
Clinical interpretation requires looking at both values together along with absolute counts of other white blood cell types to understand what’s actually happening with immune function.
Neutrophils and Other White Blood Cell Types
Neutrophils must be interpreted in context with other white blood cell types to understand the complete immune picture.
Lymphocytes are the second most abundant white blood cell type, typically 20-40% of total WBC (absolute count 1,000-4,000/μL). They include T cells, B cells, and NK cells that fight viral infections, produce antibodies, and provide long-term immune memory. The neutrophil-to-lymphocyte ratio (NLR) is calculated by dividing absolute neutrophil count by absolute lymphocyte count. Normal NLR is approximately 1-3. High NLR (above 3-4) indicates neutrophil predominance suggesting bacterial infection, chronic inflammation, stress response, or worse prognosis in various diseases (higher NLR predicts worse outcomes in cardiovascular disease, cancer, and critical illness). Low NLR (below 1) indicates lymphocyte predominance suggesting viral infection, certain leukemias, or bone marrow disorders.
Monocytes typically comprise 2-10% of total WBC (absolute count 200-1,000/μL). They differentiate into macrophages and dendritic cells in tissues, participating in phagocytosis, antigen presentation, and tissue repair. Elevated monocytes (monocytosis) occur with chronic infections (tuberculosis, endocarditis), inflammatory conditions, recovery from bone marrow suppression, and certain leukemias. Low monocytes (monocytopenia) occur with bone marrow suppression or failure.
Eosinophils typically comprise 1-6% of total WBC (absolute count 50-500/μL). They fight parasitic infections and participate in allergic reactions. Elevated eosinophils (eosinophilia) occur with allergic conditions, asthma, parasitic infections, certain medications, and autoimmune diseases. Low eosinophils occur with acute stress (cortisol suppresses eosinophils) or Cushing’s syndrome.
Basophils typically comprise 0-2% of total WBC (absolute count 0-200/μL). They release histamine and other mediators in allergic reactions. Basophilia is rare but can occur with myeloproliferative disorders or chronic inflammation.
The pattern of white blood cell abnormalities reveals specific conditions. Bacterial infection typically shows high neutrophils with normal or low lymphocytes (high NLR). Viral infection typically shows normal or low neutrophils with high lymphocytes (low NLR). Allergic conditions show high eosinophils. Bone marrow suppression shows low neutrophils, often with low lymphocytes and monocytes. Chronic inflammation shows high neutrophils with high monocytes.
Neutrophils and Inflammatory Burden
Chronic neutrophil elevation (even within “normal” range but at the higher end) reflects inflammatory burden that accelerates aging and increases disease risk.
Studies examining neutrophil count and inflammatory markers show strong correlations. Higher neutrophil counts correlate with elevated hs-CRP (high-sensitivity C-reactive protein), elevated IL-6 and other inflammatory cytokines, and markers of oxidative stress. The neutrophil-to-lymphocyte ratio (NLR) is particularly strong as an inflammatory marker—higher NLR indicates greater inflammatory burden.
Cardiovascular disease shows associations with chronic neutrophil elevation. Higher baseline neutrophil counts predict increased risk of heart attack, stroke, and cardiovascular death. Elevated NLR predicts adverse cardiovascular events independent of traditional risk factors. The association likely reflects chronic inflammation driving atherosclerosis, with neutrophils both marking and contributing to the inflammatory process.
Metabolic syndrome and insulin resistance correlate with elevated neutrophils and NLR. Visceral adiposity produces inflammatory cytokines that stimulate neutrophil production. Insulin resistance creates inflammatory environment promoting neutrophil elevation. Higher neutrophil counts and NLR predict development of diabetes in people with prediabetes.
Cancer outcomes show associations with neutrophil counts and NLR. Higher pretreatment neutrophil counts and NLR predict worse cancer survival across multiple cancer types. Elevated neutrophils in tumor microenvironment may promote cancer progression through inflammatory mechanisms. Post-diagnosis neutrophil elevation indicates worse prognosis.
All-cause mortality correlates with chronic neutrophil elevation. Population studies show that higher baseline neutrophil counts predict increased mortality from all causes over years of follow-up. The association is independent of other risk factors and suggests that chronic neutrophil elevation marks fundamental inflammatory and physiological stress.
How to Optimize Neutrophil Count
Optimizing neutrophil count requires addressing underlying causes of elevation or suppression.
For low neutrophils (neutropenia):
Review medications with your physician. Many medications can suppress neutrophils. If neutropenia developed after starting a medication, discuss alternatives. Never stop prescribed medications without medical guidance, but medication review is essential.
Correct nutritional deficiencies. Check vitamin B12—target above 400-500 pg/mL. Vegans and people with absorption issues require supplementation. Check folate and ensure adequate intake. Evaluate copper status if deficiencies in other nutrients are present. Ensure adequate protein intake for bone marrow function.
Vitamin B12 and Neutrophil Production
Vitamin B12 plays a critical role in neutrophil production because it’s required for DNA synthesis in rapidly dividing bone marrow cells. When B12 levels are low—even in the “low-normal” range—neutrophil precursors can’t mature properly, leading to chronically low or borderline neutrophil counts. This is one of the most common, overlooked causes of mild neutropenia in otherwise healthy adults, particularly in people with absorption issues, older adults, those on metformin or acid-suppressing medications, and individuals following plant-based diets. In cases where deficiency or impaired absorption is present, oral supplements may be insufficient, and intramuscular B12 injections can restore levels more reliably, supporting normal bone marrow output and immune resilience. Identifying and correcting B12 status is often one of the simplest ways to normalize neutrophils without further intervention.
Address underlying autoimmune conditions if present. Autoimmune neutropenia and conditions like lupus or rheumatoid arthritis require medical management.
Treat chronic infections. HIV, hepatitis, and other chronic viral infections can suppress neutrophils and require specific treatment.
Protect against infection if neutrophils are low. With counts below 1,000-1,500/μL, take precautions including excellent hand hygiene, avoiding sick contacts, prompt attention to fever or infection symptoms, and maintaining good dental hygiene. With severe neutropenia (below 500/μL), medical management including prophylactic antibiotics may be necessary.
Consider G-CSF treatment for severe neutropenia. In cases of severe, persistent neutropenia causing recurrent infections, granulocyte colony-stimulating factor (G-CSF) injections can stimulate neutrophil production. This requires hematology consultation and management.
For high neutrophils (neutrophilia):
Identify and treat underlying infections. Bacterial infections require appropriate antibiotic therapy. Chronic infections require specific treatment.
Address chronic inflammatory conditions. Autoimmune diseases, inflammatory bowel disease, and other inflammatory conditions require medical management. Control inflammation through disease-specific treatments.
Reduce obesity-related inflammation if present. Weight loss and improved body composition reduce chronic inflammatory burden. Visceral fat loss particularly improves inflammatory markers. Exercise regularly—reduces systemic inflammation over time. Optimize diet to minimize inflammatory foods—reduce processed foods, excess omega-6 oils, refined carbohydrates, and added sugars.
Manage stress. Chronic stress maintains elevated cortisol and neutrophil counts. Stress management techniques, adequate sleep, and lifestyle optimization reduce stress-related neutrophil elevation.
Quit smoking if applicable. Smoking causes chronic neutrophil elevation that resolves over months after cessation.
Optimize metabolic health. Improve insulin sensitivity through weight loss, exercise, and dietary optimization. Reduce hs-CRP through comprehensive metabolic optimization. Target hs-CRP below 1.0 mg/L, ideally below 0.5 mg/L.
When Neutrophil Abnormalities Require Medical Attention
Certain neutrophil findings require urgent or prompt medical evaluation.
Seek immediate medical attention if you have severe neutropenia (below 500/μL) with fever, infection symptoms, or illness—this creates risk of life-threatening infection requiring urgent treatment. Neutropenia (below 1,500/μL) with signs of severe infection including high fever, rigors, severe sore throat, mouth sores, or skin infections. Extremely high neutrophil counts (above 30,000-50,000/μL) without obvious cause—could indicate leukemia or leukemoid reaction requiring urgent workup.
Seek prompt medical evaluation (within days) if you have new neutropenia (below 1,500/μL) without obvious cause. Progressive neutrophil decline over weeks to months even if still “normal.” Neutrophilia (above 10,000-12,000/μL) persisting more than a few days without identified infection or obvious cause. Neutrophil abnormalities with other blood count abnormalities (anemia, thrombocytopenia, unusual white blood cell forms on differential). Recurrent infections, particularly bacterial or fungal, with low-normal or borderline neutrophil counts.
Routine monitoring is appropriate for stable mild neutropenia (1,500-2,500/μL) that’s been present for months to years without infections or progression—particularly if consistent with benign ethnic neutropenia. Known reactive neutrophilia from identified cause (obesity, smoking, chronic inflammation) being addressed. Mild neutrophil elevation (7,000-9,000/μL) with clear reactive cause like recent infection or stress.
Frequently Asked Questions
What is a good neutrophil count?
Optimal absolute neutrophil count is 2,500-6,000/μL, ideally 3,000-5,000/μL. Neutrophil percentage should be 45-65%, ideally 50-60%. These levels provide excellent bacterial defense without excessive inflammatory activity. Standard “normal” ranges are wider (1,500-7,800/μL), but values at the extremes often indicate suboptimal immune function or chronic inflammation.
Can low neutrophils cause fatigue?
Low neutrophils don’t directly cause fatigue—they don’t carry oxygen or affect energy production. However, underlying conditions causing neutropenia often do cause fatigue. For example, B12 deficiency causes both neutropenia and profound fatigue. Chronic infections suppressing neutrophils cause fatigue. Autoimmune conditions affecting neutrophils commonly cause fatigue through inflammation and immune activation. Additionally, if low neutrophils lead to frequent infections, the infections themselves cause fatigue.
What does it mean if neutrophils are high but total WBC is normal?
This means neutrophils comprise a higher percentage of your white blood cells than typical (above 70-75%), while other cell types (particularly lymphocytes) are proportionally reduced. This pattern suggests stress response suppressing lymphocytes while increasing neutrophils, mild chronic inflammation causing neutrophil predominance, recent viral infection recovery where lymphocytes were elevated but are declining faster than neutrophils, or early stages of infection or inflammation before total WBC rises significantly.
Is a neutrophil-to-lymphocyte ratio of 4 concerning?
NLR above 3-4 is elevated and indicates neutrophil predominance. This suggests chronic inflammation, stress response, possible bacterial infection, or increased risk of adverse outcomes in various diseases. Optimal NLR is approximately 1-3. However, NLR must be interpreted in context—temporary elevation from acute stress or recent infection is less concerning than chronic elevation. Check inflammatory markers like hs-CRP and address underlying causes of chronic inflammation.
Can exercise affect neutrophil count?
Yes, significantly. Intense exercise causes immediate neutrophil elevation through stress hormone release—counts can increase by 2,000-5,000/μL or more during and immediately after hard training. This elevation is temporary, typically resolving within hours. Chronic overtraining can suppress neutrophils over time through bone marrow stress. Moderate, consistent exercise has anti-inflammatory effects and typically improves neutrophil function without chronically elevating counts.
Why are my neutrophils low if I’m healthy and not getting sick?
Several possibilities: benign ethnic neutropenia (baseline counts of 1,000-2,500/μL in people of African, Middle Eastern, or certain other ancestries—completely normal for these individuals), individual variation (some healthy people naturally have baseline counts of 1,500-2,500/μL without increased infection risk), early nutritional deficiency (B12 or folate depletion causing mild neutropenia before other symptoms develop), or medication effects (certain drugs cause mild suppression without obvious clinical impact). If you’re truly healthy without recurrent infections, mild neutropenia may be your normal baseline. However, it’s worth checking B12, folate, and reviewing medications.
How quickly can neutrophil count change?
Very quickly. Neutrophils can increase by thousands within hours of infection, stress, or corticosteroid administration due to release of bone marrow reserves. Conversely, certain medications or overwhelming infections can drop counts within days. With chemotherapy, neutrophils typically decline 7-14 days post-treatment (nadir) and recover over the following 1-2 weeks. This rapid turnover is why neutrophils are sensitive markers of acute changes in immune status or bone marrow function.
Should I be concerned about neutrophils at 8,000/μL with no infection?
Neutrophils at 8,000/μL without acute infection suggest mild chronic inflammation, stress response (physical or psychological stress), smoking (if applicable), obesity-related inflammation, or chronic inflammatory condition. Check hs-CRP to assess inflammatory burden. Consider recent stress, illness, or lifestyle factors. If this is a one-time finding, repeat testing in 1-2 months. If chronically elevated, investigate sources of inflammation and optimize metabolic health. This level isn’t dangerous but indicates inflammatory burden worth addressing.
Testing Neutrophils With ApexBlood
ApexBlood’s comprehensive blood panel includes neutrophil count and percentage as part of the complete blood count with differential (CBC with diff), along with all related markers necessary to understand your immune function: total white blood cell count (WBC) for overall immune cell number, lymphocyte count and percentage for viral defense and NLR calculation, monocyte count and percentage for macrophage function, eosinophil count and percentage for allergic and parasitic responses, and basophil count and percentage completing the differential.
Our testing also includes critical markers that reveal what might be affecting neutrophils: high-sensitivity C-reactive protein (hs-CRP) for inflammatory assessment, vitamin B12 for bone marrow function affecting neutrophil production, ferritin and iron studies for comprehensive bone marrow nutritional status, and complete metabolic panel for kidney and liver function affecting immune health.
This comprehensive approach reveals not just your neutrophil count but the complete immune picture—whether low neutrophils reflect bone marrow suppression, autoimmune destruction, or benign ethnic variation, whether high neutrophils indicate infection, chronic inflammation, or stress response, how neutrophil-to-lymphocyte ratio reflects inflammatory burden, and whether changes over time indicate developing problems or improvement.
Neutrophil count is meaningless without context. You need to know the percentage, absolute counts of other white blood cell types, inflammatory markers like hs-CRP, and nutritional markers affecting bone marrow. You need trends over time to distinguish your baseline from acute changes.
Most doctors only check total WBC and might glance at neutrophil percentage without calculating absolute count or considering NLR. But comprehensive assessment reveals critical information about immune function, inflammatory burden, and infection risk.
You can’t optimize what you don’t measure. Stop accepting neutrophil results without understanding what they reveal about immune health, inflammation, and underlying conditions.
Get comprehensive testing including neutrophil count and complete immune assessment – $189
The Bottom Line on Neutrophils
Neutrophils are your primary defense against bacterial and fungal infections and serve as sensitive markers of immune function, inflammatory burden, bone marrow health, and stress response.
Optimal absolute neutrophil count is 2,500-6,000/μL, ideally 3,000-5,000/μL, with percentage of 45-65%, ideally 50-60%. These levels ensure excellent infection defense without excessive inflammatory activity.
Low neutrophils (neutropenia below 1,500/μL) increase infection risk and can result from medications, nutritional deficiencies (B12, folate, copper), autoimmune destruction, bone marrow disorders, viral infections, or benign ethnic variation. Severe neutropenia (below 500/μL) creates critical infection risk requiring medical management.
High neutrophils (neutrophilia above 7,000-8,000/μL) indicate bacterial infection, chronic inflammation, stress response, obesity-related inflammation, smoking, certain medications, or bone marrow disorders. Chronic elevation even within “normal” range reflects inflammatory burden that increases cardiovascular and mortality risk.
The neutrophil-to-lymphocyte ratio (NLR) provides powerful prognostic information. Optimal NLR is 1-3. Higher NLR indicates inflammatory burden and predicts worse outcomes in cardiovascular disease, cancer, and other conditions.
Neutrophils must be interpreted alongside other white blood cell types, inflammatory markers (hs-CRP), and nutritional markers (B12, folate) to understand the complete picture. Trends over time reveal developing problems or improvement more effectively than single values.
High performers track neutrophils as markers of immune function, inflammatory burden, and overall health status. They don’t just check if total WBC is “normal”—they understand that neutrophil count, percentage, and NLR provide critical information about infection risk, chronic inflammation, and long-term health outcomes.
Stop accepting neutrophil results without understanding what they reveal about your immune system and inflammatory status. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Neutrophil abnormalities require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.