
Eosinophils: The Immune Marker That Reveals Hidden Allergies, Parasites, and Chronic Inflammation
You get your CBC results back. Everything looks fine. But tucked into the differential white blood cell count is a number most people never ask about: eosinophils at 6%. Your doctor doesn’t mention it. You move on.
That’s a mistake.
Persistently elevated eosinophils are one of the immune system’s clearest distress signals – a marker that something is chronically activating your allergy and inflammation pathways. Parasitic infections, food sensitivities, environmental allergens, autoimmune activity, drug reactions, and even certain cancers can all drive eosinophil elevation long before other symptoms appear. And suppressed eosinophils tell their own story about immune compromise.
Most people have never heard of eosinophils. They don’t have the cultural familiarity of cholesterol or testosterone. But for anyone serious about understanding their immune function and controlling chronic inflammation, eosinophils are a surprisingly informative window into what’s quietly happening inside your body.
High performers don’t skip over unfamiliar biomarkers just because their doctor didn’t flag them. They understand what each number means and what it’s telling them.
What Are Eosinophils?
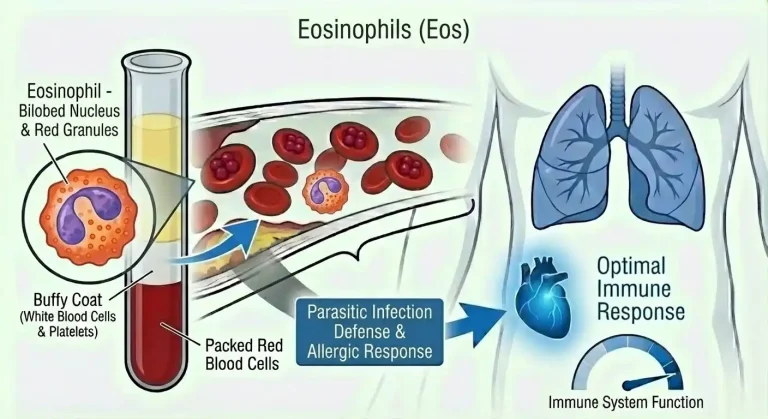
Eosinophils are a type of white blood cell produced in the bone marrow from the same precursor cells that give rise to other granulocytes – neutrophils and basophils. They make up a small fraction of circulating white blood cells in healthy individuals, typically 1-4%, but they punch well above their weight when it comes to immune function.
Their name comes from their staining characteristics in laboratory analysis – they absorb the acidic dye eosin, giving them a distinctive bright pink or red appearance under a microscope. Visually, they’re easy to identify. Functionally, they’re complex.
Eosinophils are packed with cytoplasmic granules containing a potent arsenal of inflammatory proteins: major basic protein (MBP), eosinophil peroxidase, eosinophil cationic protein (ECP), and eosinophil-derived neurotoxin. These proteins are highly toxic to parasites, bacteria, and foreign cells – which is their primary evolutionary purpose. But they’re equally toxic to healthy tissue when eosinophils are chronically activated and degranulate inappropriately, as happens in allergic and inflammatory conditions.
They circulate in the bloodstream for only about 8-12 hours before migrating into tissues – particularly the gastrointestinal tract, lungs, skin, and connective tissue – where they can survive for days to weeks. At baseline, the vast majority of eosinophils in your body are in tissues rather than circulation. What you measure in a blood test is only a small fraction of total body eosinophil activity.
Eosinophils operate primarily through two activation pathways. The allergy and parasite pathway involves IgE antibodies binding to allergens or parasitic antigens, which signals eosinophils to degranulate and attack. The cytokine pathway involves signals from T-helper cells and mast cells – particularly IL-4, IL-5, and IL-13 – that drive eosinophil production, activation, and tissue recruitment.
IL-5 is especially important. It’s the primary cytokine that stimulates bone marrow eosinophil production and prolongs eosinophil survival. Modern biologics targeting IL-5 (mepolizumab, benralizumab) are used to treat severe eosinophilic asthma and other eosinophil-driven conditions – a testament to how central IL-5 is to eosinophil biology.
Why Eosinophils Matter for Performance and Health
For most people without known allergies or parasitic exposure, eosinophils seem irrelevant. They’re not. Here’s why they matter to anyone interested in optimizing their biology.
Allergic inflammation is far more common than most people realize. Eosinophils are the primary effector cells in allergic inflammation – the cellular mechanism behind asthma, allergic rhinitis, food allergies, eczema, and a growing list of conditions classified as “eosinophilic disorders.” Many people experience chronic subclinical allergic activation without obvious symptoms – persistent low-grade nasal congestion, mild respiratory issues, skin reactivity, or gastrointestinal discomfort they’ve attributed to other causes. Elevated eosinophils at 4-8% in otherwise asymptomatic individuals often reflect this subclinical allergic load.
Systemic inflammation has performance costs. Chronic eosinophil activation contributes to the broader inflammatory environment that degrades performance – increasing fatigue, impairing recovery, disrupting sleep quality, and reducing cognitive clarity. It’s not as direct a connection as with monocytes or CRP, but persistent immune activation at any level creates inflammatory noise that impacts how you feel and function day to day.
Gastrointestinal health is directly connected to eosinophil activity. The gut is the tissue with the highest baseline eosinophil density outside of bone marrow. Conditions including eosinophilic esophagitis, eosinophilic gastroenteritis, and eosinophilic colitis are driven by abnormal gut eosinophil accumulation. These conditions are increasingly diagnosed and often present subtly – difficulty swallowing, chronic abdominal discomfort, food intolerances – without obvious systemic eosinophil elevation on blood testing.
Parasitic infection is a global reality, including in developed countries. Tissue-invasive parasites – Toxocara, Strongyloides, Trichinella, and others – can establish low-grade infections that persist for years or decades without obvious symptoms while maintaining chronically elevated eosinophils. Travel history, exposure to soil, undercooked meat, or contaminated water, and contact with animals all create exposure risk that most physicians in developed countries underestimate.
Eosinophilia is a clue to undiagnosed conditions. Elevated eosinophils on a routine CBC often represent the first visible signal of conditions that haven’t yet declared themselves clinically – autoimmune diseases, inflammatory conditions, drug reactions, and in rare cases, malignancy. Investigating elevated eosinophils rather than dismissing them often surfaces conditions that are far easier to manage when caught early.
Respiratory performance is directly impacted by eosinophilic inflammation. Eosinophilic asthma – driven by airway eosinophil accumulation – is the most common severe asthma phenotype. But subclinical airway eosinophilia can impair respiratory function and exercise capacity without meeting clinical criteria for asthma. Athletes and physically active people with unexplained respiratory limitations or exercise-induced symptoms should have eosinophils on their radar.
Normal vs. Optimal Eosinophil Levels
Standard reference ranges for eosinophils on a CBC with differential are typically:
Percentage of white blood cells: 1-4%
Absolute eosinophil count (AEC): 0.1-0.5 x 10^9/L (100-500 cells per microliter)
Eosinophilia – elevated eosinophils – is categorized by severity:
Mild eosinophilia: 500-1,500 cells/microliter (0.5-1.5 x 10^9/L)
Moderate eosinophilia: 1,500-5,000 cells/microliter
Severe (hypereosinophilia): Above 5,000 cells/microliter
The problem with “normal”: The standard range extends to 4% or 500 cells/microliter, but many healthy individuals with no allergic, infectious, or inflammatory burden show eosinophils below 2% or 200 cells/microliter. Consistently sitting at the upper end of the reference range – even technically “within normal” – often reflects chronic allergic or inflammatory activation that warrants investigation rather than reassurance.
Optimal eosinophil levels for performance and longevity:
Percentage: 1-3% of total white blood cells
Absolute count: 100-300 cells per microliter
As with monocytes, a single reading is less meaningful than a pattern. Eosinophils fluctuate – they’re elevated after allergen exposure, parasitic contact, certain foods, and some medications. They’re lowest in the morning and highest at night due to circadian cortisol variation. A consistently elevated trend across multiple measurements, or a marked single elevation, is what warrants investigation.
One important nuance: eosinophils are suppressed by cortisol. Corticosteroid treatment and high endogenous cortisol (from acute stress or Cushing’s syndrome) drive eosinophils toward zero. If you’re on corticosteroids, your eosinophil count will be artifactually low. If eosinophils are near zero without corticosteroid use, that also warrants investigation.
What Causes Elevated Eosinophils?
The causes of eosinophilia span a wide range from benign to serious, and distinguishing between them requires context.
Allergic conditions are the most common cause of mild to moderate eosinophilia in developed countries. Allergic rhinitis, asthma, atopic dermatitis (eczema), food allergies, and allergic conjunctivitis all involve chronic eosinophil recruitment and activation. People with multiple atopic conditions often show persistent eosinophilia that tracks with their allergic burden. Seasonal variation is common – eosinophils rise during high pollen periods and fall in off-season.
Food sensitivities and intolerances can maintain low-grade eosinophilic activation without producing obvious acute allergic reactions. Certain foods drive eosinophil-mediated gut inflammation – eosinophilic esophagitis, for example, is strongly linked to specific food antigens (milk, wheat, eggs, soy, nuts, and seafood are the most common triggers). The systemic eosinophil count may be normal even when localized gut eosinophilia is significant.
Parasitic infections are the most common cause of significant eosinophilia worldwide. Tissue-invasive parasites are the key drivers – intestinal parasites that stay confined to the gut lumen (like Giardia) don’t typically elevate eosinophils, but those that migrate through tissues do. Toxocara (from contact with dog or cat feces), Strongyloides (from soil contact in endemic regions), Trichinella (from undercooked pork or wild game), hookworm, and numerous other tissue-invasive helminths maintain eosinophilia for the duration of infection. In travelers or people with rural or international exposure history, parasitic causes must be actively ruled out.
Drug reactions are an underappreciated cause of eosinophilia. Many medications can trigger eosinophilic reactions – NSAIDs, certain antibiotics (particularly sulfonamides and ampicillin), anticonvulsants, allopurinol, and many others. Drug reaction with eosinophilia and systemic symptoms (DRESS syndrome) is a severe, potentially life-threatening reaction that includes marked eosinophilia alongside rash and organ involvement. Any new eosinophilia in the setting of a recently started medication deserves serious attention.
Autoimmune and inflammatory conditions including eosinophilic granulomatosis with polyangiitis (formerly Churg-Strauss syndrome), inflammatory bowel disease, rheumatoid arthritis, and sarcoidosis can produce significant eosinophilia. These conditions involve immune dysregulation that drives eosinophil production and tissue recruitment.
Eosinophilic disorders are conditions defined by abnormal eosinophil accumulation in specific tissues – eosinophilic esophagitis (EoE), eosinophilic gastroenteritis, eosinophilic pneumonia, and hypereosinophilic syndrome (HES). Peripheral blood eosinophilia may be mild or even absent in some localized eosinophilic disorders, making tissue biopsy necessary for diagnosis.
Skin conditions including eczema, psoriasis, and other inflammatory dermatoses involve eosinophil-mediated tissue damage and often produce mild systemic eosinophilia.
Malignancy in rare cases drives eosinophilia. Hodgkin’s lymphoma is classically associated with eosinophilia, as are some solid tumors that secrete cytokines stimulating eosinophil production. Eosinophilic leukemia – a rare primary bone marrow malignancy – causes dramatic eosinophil overproduction. Marked, unexplained eosinophilia (above 1,500 cells/microliter) without an obvious allergic or infectious explanation should prompt evaluation for underlying malignancy.
Adrenal insufficiency reduces cortisol, which normally suppresses eosinophil counts. People with Addison’s disease or secondary adrenal insufficiency often show elevated eosinophils as a reflection of inadequate cortisol activity. Persistently elevated eosinophils alongside fatigue, low blood pressure, and salt cravings should include adrenal function in the differential.
Chronic stress and poor sleep can contribute to eosinophil dysregulation. While acute stress elevates cortisol and suppresses eosinophils, the complex hormonal environment of chronic stress can alter immune regulation in ways that allow eosinophil elevation, particularly when allergic sensitization is already present.
What Causes Low Eosinophils?
Eosinopenia – eosinophil counts below 100 cells per microliter – is less discussed but significant.
Corticosteroid use is the most common cause. Exogenous corticosteroids (prednisone, dexamethasone, inhaled corticosteroids at high doses) directly suppress eosinophil production and survival, driving counts toward zero. This is expected and not pathological in the context of corticosteroid therapy.
Acute infection and stress drive cortisol elevation that transiently suppresses eosinophils. This is part of the normal acute stress response. Eosinophils typically return to baseline within days after the acute stressor resolves.
Cushing’s syndrome – pathological cortisol excess from adrenal tumors or pituitary disease – chronically suppresses eosinophils alongside producing the classic constellation of central obesity, hypertension, glucose dysregulation, and muscle wasting.
Bone marrow suppression from chemotherapy, radiation, or primary marrow disorders reduces all white blood cell lines including eosinophils.
Sepsis in severe cases can deplete eosinophils as part of the profound immune dysregulation accompanying critical illness.
Persistently low or absent eosinophils outside of corticosteroid use or acute illness warrant evaluation for the above conditions. Isolated eosinopenia in an otherwise healthy person on no medications is unusual and worth investigating.
How to Optimize Eosinophil Levels
When eosinophils are elevated, optimization means identifying and addressing the underlying driver – not just managing the number.
Identify and reduce allergen exposure. If allergic conditions are driving elevation, the most effective intervention is reducing the allergenic burden. Environmental allergen testing identifies specific sensitizations. Common culprits include dust mites, pet dander, mold, and pollen. Reducing exposure through environmental controls – HEPA filtration, mattress covers, humidity management – produces measurable reductions in eosinophilic inflammation over time.
Investigate and address food triggers. If food sensitivities are suspected, a structured elimination protocol – removing the most common allergenic foods for 4-6 weeks and monitoring both symptoms and eosinophil counts – can identify dietary drivers. Working with a physician experienced in food-related immune activation provides the most reliable results.
Rule out parasitic infection. If eosinophils are persistently elevated – particularly above 500 cells/microliter – and you have any relevant exposure history (international travel, rural environments, contact with animals, consumption of undercooked meat), parasitic screening is warranted. Stool ova and parasite testing, serology for Toxocara and Strongyloides, and in some cases empirical treatment for Strongyloides (which can persist for decades) should be considered.
Review medications. Any elevated eosinophils in the setting of recently started medications deserves a review with your physician. Drug-induced eosinophilia typically resolves within weeks of stopping the offending agent.
Optimize immune regulation through lifestyle. The same interventions that reduce chronic inflammation broadly also tend to normalize eosinophilic activity – anti-inflammatory diet, quality sleep, stress management, and regular exercise. Omega-3 fatty acids have specific evidence for modulating eosinophil-driven inflammation through their effects on arachidonic acid metabolism and inflammatory eicosanoid production.
Vitamin D optimization is relevant here. Vitamin D plays a direct role in immune regulation, including modulation of the Th2-skewed immune response that drives eosinophil activation. Vitamin D deficiency is associated with higher allergic disease burden and elevated eosinophils. Optimal vitamin D levels (50-70 ng/mL) support appropriate immune balance.
Address gut health. Given the density of eosinophils in gastrointestinal tissue and the role of gut immune dysregulation in eosinophilic disorders, gut health optimization is directly relevant. A diverse, fiber-rich diet that supports a healthy microbiome, avoidance of known food triggers, and in some cases targeted gut-healing protocols reduce eosinophilic gut inflammation.
Eosinophils and Other Health Markers
Eosinophils become most informative when viewed alongside related immune and inflammatory markers.
IgE (immunoglobulin E) is the antibody class central to allergic responses. Elevated total IgE alongside elevated eosinophils strongly suggests allergic sensitization as the driver. Specific IgE testing for individual allergens identifies the precise triggers.
hs-CRP contextualizes the inflammatory picture. Elevated eosinophils with elevated hs-CRP suggests significant systemic inflammation. Normal hs-CRP with elevated eosinophils may indicate a more localized eosinophilic process or lower-grade allergic activation.
Complete blood count differential provides the full white blood cell context. Elevated eosinophils alongside elevated basophils (another granulocyte heavily involved in allergy) strongly implicates allergic activation. Eosinophilia alongside lymphocytosis may suggest viral infection or autoimmune disease.
Tryptase is a mast cell marker that rises with mast cell activation – which often accompanies eosinophil activation in allergic conditions. Elevated tryptase alongside eosinophilia suggests significant allergic immune activation.
Stool testing – including ova and parasites, and in some cases comprehensive stool analysis – complements blood eosinophil measurement when parasitic or gastrointestinal inflammatory causes are suspected.
Vitamin D levels are worth checking alongside eosinophil elevation given the established connection between vitamin D status and Th2-skewed immune dysregulation driving eosinophil activation.
Cortisol – either serum morning cortisol or a 24-hour urinary cortisol – is relevant when eosinophilia is persistent and unexplained, to evaluate adrenal function.
Frequently Asked Questions
What does it mean if my eosinophils are slightly elevated?
Mild elevation (4-8%, or 500-800 cells/microliter) most commonly reflects subclinical allergic activation, seasonal allergen exposure, or food sensitivities in otherwise healthy adults in developed countries. A single mildly elevated reading without other symptoms or inflammatory markers is often not alarming – but a persistently elevated pattern across multiple tests warrants investigation for the underlying driver, whether allergic, infectious, or inflammatory.
Can eosinophils indicate food sensitivity?
Yes, though the relationship is indirect. Food-allergic eosinophilic inflammation often occurs primarily in gut tissues, where blood eosinophil counts may not fully reflect what’s happening locally. Eosinophilic esophagitis, for example, is diagnosed by esophageal biopsy, not blood tests. That said, significant food-driven immune activation can produce mild systemic eosinophilia, and elimination protocols often produce measurable improvements in eosinophil counts alongside symptom resolution.
Should I be tested for parasites if my eosinophils are elevated?
If your eosinophils are consistently above 500 cells/microliter without a clear allergic or drug-related cause, and particularly if you have any history of international travel, rural or soil exposure, animal contact, or consumption of undercooked meat, parasitic screening is a reasonable next step. Strongyloides in particular can persist for decades without obvious symptoms and is often missed on standard stool testing – serology is more sensitive.
Do eosinophils go up with seasonal allergies?
Yes. Seasonal allergen exposure – pollen, mold spores – drives eosinophil elevation that tracks with allergy season. People with seasonal allergic rhinitis or asthma often show eosinophil elevation during peak season that resolves in off-season periods. If you’re testing eosinophils for baseline purposes, testing outside of your known allergy season provides a more accurate baseline.
Can exercise affect eosinophil counts?
Moderate exercise has a modest suppressive effect on eosinophils through cortisol release. Intense exercise can temporarily elevate inflammatory markers broadly. Exercise-induced bronchoconstriction – which affects a significant proportion of endurance athletes – involves airway eosinophilia that may or may not reflect in peripheral blood counts. Athletes with unexplained respiratory limitations during exercise should have eosinophils and allergy markers assessed.
What is hypereosinophilic syndrome?
Hypereosinophilic syndrome (HES) is defined by eosinophils consistently above 1,500 cells/microliter for more than one month, with evidence of eosinophil-mediated organ damage (heart, lungs, skin, nervous system) and no secondary cause identified. It’s rare but serious – the combination of high eosinophil counts and tissue infiltration can cause progressive organ damage, particularly cardiac damage. Any persistent eosinophilia above 1,500 cells/microliter requires thorough medical evaluation.
Are elevated eosinophils dangerous?
Mild, transient elevation from allergic or infectious causes is generally not dangerous and resolves with the underlying trigger. Persistent moderate-to-severe elevation (above 1,500 cells/microliter) carries risk of eosinophil-mediated tissue damage – particularly cardiac (Loeffler endocarditis), pulmonary, and neurological complications – regardless of cause. The severity of risk scales with the degree and duration of eosinophilia.
Can eosinophils be a sign of cancer?
Rarely, yes. Hodgkin’s lymphoma, certain solid tumors, and eosinophilic leukemia can all drive eosinophilia. This is an uncommon cause of elevated eosinophils relative to allergic and infectious causes, but persistent significant eosinophilia (above 1,000-1,500 cells/microliter) without an identified allergic or infectious explanation warrants evaluation that includes ruling out malignancy.
Testing Eosinophils With ApexBlood
Eosinophils are reported as part of the CBC with differential included in ApexBlood’s comprehensive blood panel. But like every immune marker, they tell their most useful story alongside the context that explains them – total IgE, hs-CRP, vitamin D, full immune differential, and the metabolic markers that reveal whether systemic inflammation is at the root.
A single eosinophil number without context is a starting point, not an answer. Comprehensive testing reveals the complete immune and inflammatory picture – whether eosinophil elevation is part of a broader inflammatory pattern, whether it’s isolated and allergy-driven, or whether it’s a signal pointing toward something that needs further investigation.
Most physicians check a CBC reactively when you’re symptomatic. High performers test proactively, establish baselines across all immune markers, and track changes over time – because immune dysregulation is far easier to address when it’s caught early, not after it’s declared itself as disease.
Get comprehensive testing – $189
The Bottom Line on Eosinophils
Eosinophils are your immune system’s primary allergy and anti-parasite responders, and their count reflects the cumulative allergic, infectious, and inflammatory burden your body is carrying. Most people never look at this number. That’s a missed opportunity.
Optimal eosinophils are 1-3% of white blood cells (100-300 cells per microliter). Persistently elevated counts – even technically “within normal” range – often reflect chronic allergic activation, subclinical infection, food sensitivities, or drug reactions that are silently maintaining inflammatory immune activity. Significant elevation above 500-1,000 cells/microliter without an obvious cause demands investigation.
Optimizing eosinophils means addressing root causes – identifying and reducing allergen exposure, investigating parasitic infection when warranted, reviewing medications, optimizing vitamin D and gut health, and reducing the overall inflammatory burden that keeps immune cells in a state of chronic low-grade activation.
High performers don’t leave immune markers unexamined. They know that chronic immune activation – at whatever level and through whatever mechanism – creates biological noise that degrades performance, disrupts recovery, and accelerates inflammatory aging.
You can’t optimize what you don’t measure. Stop accepting chronically elevated immune activation when the underlying driver is often identifiable and addressable.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Eosinophil levels and immune health require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.