
Basophils: The Rarest White Blood Cell That Reveals the Most About Allergic Inflammation
Your CBC results show basophils at 0.0%. Your doctor doesn’t mention it. You assume zero means fine and move on.
But basophils aren’t supposed to be zero – and when they are, it means something. And when they’re elevated, even slightly, that also means something. Basophils occupy a tiny fraction of your circulating white blood cells, but they’re disproportionately powerful players in allergic inflammation, immune regulation, and the chronic inflammatory states that quietly degrade performance and longevity.
They’re the least understood and least discussed of all white blood cells. Most physicians glance at basophils, note they’re “within range,” and move on without a second thought. But for anyone serious about understanding their immune biology, basophils are worth understanding – because even small shifts in this marker carry signal that other white blood cell counts don’t.
High performers don’t skip the markers their doctors overlook. They understand what every number means and what it’s telling them.
What Are Basophils?
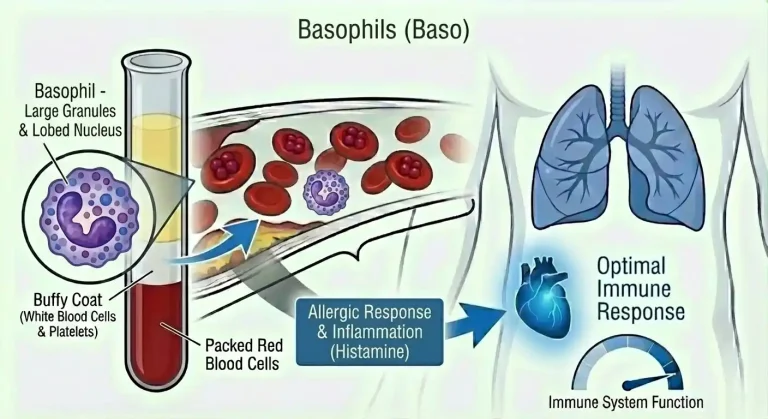
Basophils are granulocytes – white blood cells characterized by large granules in their cytoplasm that contain powerful inflammatory mediators. They’re produced in the bone marrow from the same progenitor cells as other granulocytes and circulate in the bloodstream for only 1-2 days before migrating into tissues.
They are, by count, the rarest white blood cell in circulation. In healthy adults, basophils represent less than 1% of all circulating white blood cells – typically 0.5-1.0% on a CBC with differential, translating to roughly 20-100 cells per microliter of blood. The absolute numbers are so small that even minor fluctuations in cell counts produce large percentage swings, which is why basophil results require careful interpretation.
What basophils lack in quantity, they make up for in biochemical firepower. Their granules are densely packed with histamine, heparin, serotonin, leukotrienes, and prostaglandins – the same potent inflammatory mediators found in mast cells, their tissue-resident cousins. When basophils degranulate – releasing their granule contents in response to activation – the resulting inflammatory cascade is immediate and powerful.
The relationship between basophils and mast cells is important context. They share a common progenitor, express many of the same surface receptors, carry similar granule contents, and serve overlapping functional roles in allergy and inflammation. The primary distinction is location: basophils circulate in blood, while mast cells reside in tissues – particularly skin, gut, lungs, and connective tissue. When you experience an allergic reaction, both cell types are typically involved.
Central to basophil function is the high-affinity IgE receptor (FcεRI) expressed on their surface. IgE antibodies – produced in response to allergen sensitization – bind to these receptors. When the allergen the IgE recognizes is encountered again, it cross-links the surface IgE, triggering immediate basophil degranulation. This is the mechanism behind immediate allergic reactions – the rapid onset of symptoms within minutes of allergen exposure.
But basophils aren’t purely reactive cells that sit dormant until allergen exposure. They also produce cytokines including IL-4, IL-13, and TSLP that actively shape the broader immune environment – promoting the Th2-skewed immune polarization that underlies allergic disease, recruiting other immune cells to sites of inflammation, and influencing the intensity and chronicity of allergic responses.
Why Basophils Matter for Performance and Health
Given how few circulating basophils exist at any given time, it’s tempting to dismiss them as biologically minor. That would be a mistake.
Allergic inflammation is orchestrated in part by basophils. When you’re exposed to an allergen, basophils are among the first responders – degranulating within seconds to minutes, releasing histamine that drives the immediate symptoms of allergic reactions: swelling, itching, redness, bronchoconstriction, and in severe cases, anaphylaxis. For the estimated 30-40% of people with some degree of allergic sensitization, basophil reactivity is directly relevant to how they experience daily life.
But the impact of basophil-driven allergic inflammation extends beyond obvious allergic reactions. Chronic subclinical allergic activation – below the threshold of noticeable symptoms – maintains a low-grade inflammatory environment that affects sleep quality, cognitive clarity, energy levels, and recovery. People who dismiss mild perennial allergic symptoms as their “normal” baseline are often carrying an immune burden that, when addressed, produces meaningful improvements in how they feel and perform.
Histamine release has systemic effects beyond allergic symptoms. Histamine released by basophils (and mast cells) affects multiple systems simultaneously. In the central nervous system, histamine influences arousal, alertness, and sleep-wake cycling – histamine H1 receptor antagonists (antihistamines) cause sedation precisely because blocking histamine signaling promotes drowsiness. In the cardiovascular system, histamine causes vasodilation and increased vascular permeability. In the gastrointestinal system, it stimulates acid secretion and affects motility. People with chronically activated basophils and elevated histamine release often experience systemic effects – brain fog, disrupted sleep architecture, GI symptoms, and fatigue – that they rarely connect to immune activation.
Basophils are sentinels of allergic disease severity. Research consistently shows that basophil reactivity – how easily basophils degranulate in response to allergen exposure – correlates with the clinical severity of allergic disease. People with highly reactive basophils experience more severe allergic responses to the same allergen load compared to those with less reactive basophils. Basophil activation testing (BAT), a specialized assay not included in standard CBCs, directly measures basophil reactivity and is increasingly used in clinical allergy evaluation.
The connection between basophils and chronic disease is emerging. Beyond their established role in allergy, basophils are increasingly recognized as participants in autoimmune disease, inflammatory conditions, and even tumor immunity. They interact with T regulatory cells, B cells, and dendritic cells in ways that influence whether the immune system mounts appropriate or dysregulated responses. Persistently elevated basophils in people without obvious allergic disease often reflect broader immune dysregulation worth investigating.
Basophils as a longevity marker. Emerging research on biological aging and immune senescence shows that shifts in white blood cell differential – including basophil counts – correlate with inflammatory aging trajectories. Chronically elevated basophils contributing to allergic inflammation accelerate the inflammatory aging process. Optimizing immune balance, including keeping allergic inflammation appropriately controlled, is increasingly recognized as a component of longevity strategy.
Normal vs. Optimal Basophil Levels
Standard reference ranges for basophils on a CBC with differential are typically:
Percentage of white blood cells: 0-1%
Absolute basophil count (ABC): 0-100 cells per microliter (0.0-0.1 x 10^9/L)
These ranges reflect just how sparse basophils are in circulation under normal conditions. The upper limit of 1% is already quite generous – most healthy individuals with low allergic burden and minimal chronic inflammation show basophils at 0.5% or below.
Basophilia – elevated basophils – is defined as an absolute count above 100-110 cells per microliter or a percentage above 1%. Even mild basophilia is worth noting given the small baseline numbers involved. A shift from 0.5% to 1.5% represents a tripling of basophil count, even though the absolute number remains small.
The nuance of near-zero basophils: A reading of 0.0% or 0-20 cells per microliter is commonly reported and often means nothing more than that basophils were too few to register meaningfully on that particular draw. Because circulating basophil numbers are so small, they’re prone to statistical variation – day-to-day fluctuation is normal. A single reading of zero in an otherwise healthy person on no medications is not inherently alarming.
However, persistently absent basophils – particularly alongside clinical signs of immune compromise or in the setting of systemic illness – can be significant, as discussed in the low basophil section below.
Optimal basophil levels for performance and longevity:
Percentage: 0.2-0.8% of total white blood cells
Absolute count: 20-80 cells per microliter
The goal isn’t a specific number so much as stability within a low, normal range alongside absence of symptoms suggesting allergic or histamine-mediated immune dysregulation. Context from other immune markers – eosinophils, IgE, hs-CRP – matters enormously for interpreting basophil counts correctly.
What Causes Elevated Basophils?
Basophilia is uncommon relative to elevation of other white blood cells, which makes it a more specific signal when it occurs. Understanding what drives it is essential for correct interpretation.
Allergic conditions are the most common cause of mild basophilia in otherwise healthy people. Chronic allergic rhinitis, allergic asthma, atopic dermatitis, food allergies, and other IgE-mediated conditions maintain ongoing basophil activation and can produce mild persistent elevation. Basophilia often tracks with eosinophilia in allergic individuals – seeing both elevated together strongly implicates allergic immune activation.
Inflammatory conditions including inflammatory bowel disease, rheumatoid arthritis, and other autoimmune conditions can elevate basophils as part of broader immune dysregulation. Basophils interact with multiple immune cell populations involved in autoimmunity, and their elevation in these contexts reflects active inflammatory immune activity.
Chronic infection – particularly certain viral infections and chronic parasitic infestations – can produce mild basophilia alongside more prominent eosinophilia. Like eosinophils, basophil elevation in the setting of chronic infection reflects ongoing immune engagement.
Hypothyroidism has a well-documented association with basophilia. Thyroid hormone directly influences basophil production and activity – when thyroid function is low, basophil counts tend to rise. This connection is clinically useful: unexplained mild basophilia should prompt thyroid function testing, including TSH, free T3, and free T4. Treating hypothyroidism often normalizes basophil counts without any direct immune intervention.
Iron deficiency is associated with basophilia through mechanisms that are not fully characterized but are consistently observed clinically. Correcting iron deficiency – confirmed by ferritin assessment – often normalizes basophil counts that were mildly elevated.
Myeloproliferative neoplasms are the most clinically serious cause of significant basophilia and deserve particular attention. Chronic myelogenous leukemia (CML), polycythemia vera, essential thrombocythemia, and myelofibrosis – collectively the classic myeloproliferative neoplasms – frequently produce marked basophilia, often above 2-3% with absolute counts well above normal. Basophilia is actually one of the diagnostic features of CML, and significant unexplained basophilia should always prompt evaluation to rule out these conditions. The BCR-ABL fusion gene driving CML also directly stimulates basophil production, making basophilia a particularly characteristic feature.
Estrogen influences basophil counts, which explains why some women notice changes in basophil levels across their menstrual cycle. Estrogen promotes basophil production and degranulation, which is one reason allergic conditions often worsen premenstrually when estrogen fluctuates.
Certain medications can elevate basophils. Estrogen-containing hormonal medications, antithyroid drugs, and some biologics have been associated with basophil count changes.
Food and environmental allergen exposure transiently elevates basophils in sensitized individuals following exposure to their specific allergens. This is a reactive, expected immune response rather than a pathological finding – but persistent low-level exposure to unidentified allergens can maintain chronically mildly elevated basophils that resolve once the trigger is identified and removed.
What Causes Low Basophils?
Basopenia – basophil counts below 20 cells per microliter, or near zero – is actually quite common as a laboratory finding, though true pathological basopenia is less frequent than the zero readings that appear on routine CBCs.
Acute allergic reactions and anaphylaxis cause a paradoxical drop in circulating basophils. When an immediate allergic reaction occurs, basophils rapidly migrate out of circulation into tissues and degranulate at the reaction site, depleting circulating numbers. The basophil count in the hours following an anaphylactic episode can be near zero, recovering over the subsequent 24-72 hours. This is one clinical scenario where a zero basophil count is directly meaningful rather than a statistical artifact.
Corticosteroids suppress basophil production and survival, driving counts toward zero. This is the same mechanism seen with eosinophils – cortisol broadly suppresses granulocyte populations involved in allergy. Patients on systemic corticosteroids, and to a lesser degree inhaled corticosteroids at high doses, routinely show basophil counts at or near zero.
Acute infection and stress response elevates cortisol, which transiently suppresses basophils. During acute febrile illness or significant physiological stress, basophils may drop to near zero as part of the normal acute-phase response, recovering as the stressor resolves.
Hyperthyroidism produces the opposite effect from hypothyroidism on basophil counts – elevated thyroid hormone is associated with basopenia. Like hypothyroidism-related basophilia, this relationship makes thyroid function an important consideration when basophil counts are persistently abnormal in either direction.
Ovulation and pregnancy are associated with reduced basophil counts in some women. The hormonal environment of the luteal phase and pregnancy shifts immune balance in ways that tend to suppress basophil production.
Bone marrow suppression from chemotherapy, radiation, or primary marrow disease reduces all granulocyte populations including basophils.
Urticaria (chronic hives) is associated with basopenia in a clinically important and somewhat counterintuitive way. People with chronic spontaneous urticaria – hives persisting for more than six weeks without an obvious trigger – often show reduced circulating basophils because basophils are constitutively activated and continuously migrating out of circulation into skin tissues. Paradoxically, basopenia can be a marker of significant mast cell and basophil-driven disease rather than immune quiescence.
How to Optimize Basophil Levels
Optimizing basophils follows the same principle as other immune markers – the goal is addressing the underlying driver, not chasing a number.
Identify and eliminate allergen triggers. When basophilia reflects chronic allergic activation, systematic allergen identification is the most impactful intervention. Comprehensive allergy testing – environmental and food allergen-specific IgE panels, or skin prick testing – identifies sensitizations. Reducing exposure through environmental controls (HEPA filtration, dust mite encasements, pet dander management) and dietary elimination of confirmed food allergens reduces the ongoing IgE-mediated stimulation keeping basophils elevated.
Evaluate thyroid function. Given the well-established connection between thyroid status and basophil counts, any unexplained basophilia or basopenia should include comprehensive thyroid assessment – TSH, free T3, free T4, and thyroid antibodies (TPO and TgAb). Optimizing thyroid function frequently normalizes basophil counts as a secondary benefit.
Check iron status. Ferritin should be evaluated alongside basophil elevation. If iron stores are suboptimal (ferritin below 50 ng/mL), iron repletion is a straightforward intervention that often normalizes mild basophilia. Don’t supplement iron without confirmed deficiency – excess iron carries its own risks.
Optimize vitamin D. Vitamin D is a direct modulator of immune balance, including the Th2-skewed immune polarization that drives basophil and mast cell activation. People with vitamin D deficiency (below 30 ng/mL) consistently show higher allergic disease burden and more dysregulated immune function. Optimizing vitamin D to 50-70 ng/mL supports appropriate immune regulation and often reduces allergic immune activation over time.
Reduce total allergic burden through diet and lifestyle. An anti-inflammatory dietary pattern reduces the background inflammatory environment that amplifies basophil reactivity. Omega-3 fatty acids specifically modulate the production of inflammatory eicosanoids that basophils and mast cells rely on during degranulation. Quercetin – found in onions, apples, capers, and berries – has well-documented mast cell and basophil-stabilizing properties, reducing spontaneous degranulation without eliminating appropriate immune responses.
Manage chronic stress. The complex hormonal environment of chronic psychological stress dysregulates immune balance in ways that can amplify allergic reactivity. While acute stress temporarily suppresses basophils through cortisol, the chronic stress milieu – with dysregulated HPA axis activity and disrupted circadian cortisol patterns – can paradoxically promote allergic sensitization and immune dysregulation over time.
Prioritize sleep quality. Histamine – released by basophils and mast cells – directly influences sleep architecture through its effects on arousal pathways. People with allergic conditions and elevated histamine release often experience disrupted sleep characterized by difficulty initiating sleep, frequent nocturnal arousal, and non-restorative sleep. Reducing allergic immune activation improves sleep quality, and better sleep in turn reduces the cortisol dysregulation that perpetuates immune imbalance. The relationship is bidirectional and reinforcing.
Rule out and address myeloproliferative conditions. If basophilia is persistent and significant – above 1.5-2% or above 100-150 cells per microliter without an obvious allergic, inflammatory, or thyroid explanation – evaluation to rule out myeloproliferative neoplasms is essential. This includes a comprehensive CBC, peripheral blood smear evaluation, and in some cases bone marrow assessment. This is not a lifestyle optimization question – it requires medical evaluation.
Basophils and Other Health Markers
Basophils are most informative alongside related markers that reveal the immune and inflammatory context driving any abnormality.
Eosinophils are the most important companion marker. Basophilia and eosinophilia co-occur consistently in allergic conditions, and seeing both elevated together strongly implicates allergic immune activation as the common driver. When basophils are elevated but eosinophils are normal, the differential expands to include myeloproliferative disease, hypothyroidism, or iron deficiency rather than pure allergic activation.
Total IgE and allergen-specific IgE confirm whether allergic sensitization underlies basophil elevation. Elevated total IgE alongside basophilia makes allergic activation the most probable explanation. Normal IgE with elevated basophils shifts suspicion toward non-allergic causes.
hs-CRP contextualizes the inflammatory picture. Elevated basophils with elevated hs-CRP suggest systemic inflammatory activation. Normal hs-CRP with mild basophilia may indicate lower-grade allergic activation without significant downstream systemic inflammation.
TSH, free T3, free T4 are essential when basophil counts are persistently abnormal in either direction. Thyroid function is the most frequently overlooked cause of basophil abnormalities and the one most easily addressed when identified.
Ferritin and iron studies evaluate iron status when basophilia lacks an obvious allergic explanation.
Complete blood count with differential provides critical context. The full white blood cell picture matters – basophilia alongside elevated neutrophils, eosinophils, and potentially elevated platelets or red blood cells raises concern for myeloproliferative disease. Isolated mild basophilia in an otherwise normal CBC is a much more reassuring finding.
Tryptase – a mast cell marker – rises with significant mast cell activation and often parallels basophil activation in allergic responses. Elevated tryptase alongside basophilia indicates substantial allergic immune mobilization.
Vitamin D is worth checking alongside any immune dysregulation, including basophil abnormalities, given its broad immunomodulatory role.
Frequently Asked Questions
What does it mean if my basophils are 0%?
It depends on context. A single reading of 0% or near-zero basophils is extremely common and often represents normal statistical variation – basophil numbers are so small that they can fall below detection threshold on a given draw without any pathological meaning. However, persistently zero basophils in someone not on corticosteroids, or zero basophils following a severe allergic reaction, or zero basophils alongside other immune abnormalities, warrants further investigation. Don’t panic about a single zero reading, but don’t dismiss a persistent pattern either.
Are basophils related to allergies?
Directly and centrally. Basophils are primary effector cells in IgE-mediated allergic responses – they carry high-affinity IgE receptors, degranulate rapidly upon allergen exposure, and release histamine and other mediators that produce allergic symptoms. Elevated basophils often reflect chronic allergic activation, and basophil reactivity tracks with allergic disease severity. If you have elevated basophils alongside elevated eosinophils and elevated IgE, allergic disease is almost certainly the driver.
What is the connection between basophils and histamine intolerance?
Basophils are one of the primary histamine-releasing cells in the body. People with histamine intolerance – characterized by symptoms including headaches, flushing, itching, GI distress, and brain fog following histamine-rich foods or histamine-releasing triggers – often have chronically activated basophils and mast cells releasing histamine at baseline. This isn’t a true allergy but rather an imbalance between histamine load (from food, immune cells, and gut bacteria) and histamine clearance capacity (primarily through the enzyme diamine oxidase). Addressing basophil and mast cell activation is part of managing histamine intolerance.
Should I be worried about basophils and leukemia?
Significant, persistent basophilia – above 1.5-2% or absolute counts consistently above 100-150 cells/microliter without an obvious allergic, thyroid, or inflammatory explanation – warrants medical evaluation to rule out myeloproliferative conditions including CML. This doesn’t mean that elevated basophils equal leukemia – far from it. Allergic conditions, hypothyroidism, and iron deficiency are far more common causes of mild basophilia. But because significant unexplained basophilia is one of the diagnostic features of CML, it deserves proper evaluation rather than watchful waiting. Your physician can stratify risk appropriately based on the full CBC picture.
Can diet affect basophil counts?
Indirectly, yes. Diet influences basophil activity through multiple pathways. Foods that trigger IgE-mediated responses in sensitized individuals cause basophil activation and can maintain elevated counts with repeated exposure. Anti-inflammatory dietary patterns reduce the background inflammatory environment that amplifies basophil reactivity. Histamine-rich foods (fermented foods, aged cheeses, wine, cured meats) directly burden histamine clearance pathways and can worsen symptoms in people with basophil and mast cell overactivation, even without changing circulating basophil numbers.
Why do women sometimes have higher basophils?
Estrogen promotes basophil production and degranulation, creating hormonally-driven variation in basophil counts. Many women notice worsening allergic symptoms premenstrually or at specific cycle phases – this often reflects estrogen-driven basophil and mast cell activation. Women with conditions involving estrogen excess or fluctuation (PCOS, perimenopause, estrogen-containing medications) may show consistently higher basophil activity.
How do basophils differ from mast cells?
They’re closely related – sharing a common progenitor, similar granule contents, and overlapping functions in allergic and inflammatory responses. The primary distinction is location and lifespan. Basophils circulate in blood for 1-2 days before migrating into tissues and dying. Mast cells are long-lived tissue residents that don’t normally circulate in blood – they reside in skin, gut, lungs, and connective tissue for months to years. When you experience an immediate allergic reaction, both are typically activated simultaneously. When you have a localized tissue reaction – a bug bite, food sensitivity reaction in the gut, contact dermatitis – mast cells are doing most of the local work. Blood basophil counts reflect circulating immune activity, while mast cell activity is better assessed through tissue biopsy or serum tryptase.
Can stress cause elevated basophils?
The relationship between stress and basophils is complex. Acute stress elevates cortisol, which suppresses basophils. Chronic stress with dysregulated cortisol patterns can promote allergic immune sensitization and amplify basophil reactivity over time through less direct mechanisms – disrupting circadian immune rhythms, altering gut permeability in ways that increase allergen exposure, and shifting immune balance toward Th2 dominance. People with chronic high-stress lifestyles often carry a higher allergic burden and more activated basophil biology, even if their acute cortisol response is blunted from chronic HPA axis dysregulation.
Testing Basophils With ApexBlood
Basophils are included as part of the CBC with differential in ApexBlood’s comprehensive blood panel. But because basophils tell their most useful story in context – alongside eosinophils, IgE, thyroid markers, ferritin, hs-CRP, and the full immune picture – comprehensive testing is what allows meaningful interpretation rather than isolated number-chasing.
A single basophil percentage without context is nearly uninterpretable. Is it elevated because of allergic activation, thyroid dysfunction, iron deficiency, or something more serious? Is it low because of corticosteroid use, an acute allergic reaction, or hyperthyroidism? The answer requires surrounding data – and that’s exactly what comprehensive testing provides.
Most physicians note basophil counts as an afterthought on a CBC and move on. High performers understand that even the least-discussed immune markers carry signal – and that patterns across multiple markers over time reveal what single snapshots cannot.
Get comprehensive testing – $189
The Bottom Line on Basophils
Basophils are the smallest population of white blood cells in circulation, but they’re disproportionately important in allergic inflammation, histamine biology, and immune regulation. They’re rarely discussed and routinely overlooked – which means the signal they carry often goes unread.
Optimal basophils are 0.2-0.8% of white blood cells (20-80 cells per microliter). Elevation above 1% warrants investigation – most commonly for allergic conditions, hypothyroidism, or iron deficiency, and in cases of significant persistent elevation, for myeloproliferative disease. Near-zero readings are often statistical noise but carry meaning in the context of acute allergic reactions, corticosteroid use, or hyperthyroidism.
The chronic low-grade allergic inflammation that basophil overactivation drives has real performance consequences – disrupted sleep from histamine-mediated arousal, cognitive fog from systemic inflammatory signaling, impaired recovery from chronic immune activation. These effects are subtle enough that most people attribute them to other causes and never connect them to immune function.
Optimizing basophils means identifying allergen triggers, supporting thyroid function, ensuring adequate iron and vitamin D, and reducing the total inflammatory burden that keeps immune cells in a state of chronic reactivity.
High performers understand that immune health isn’t just about preventing infection – it’s about maintaining appropriate immune balance that doesn’t silently tax energy, cognitive function, and recovery day after day.
You can’t optimize what you don’t measure. Stop overlooking the markers your doctor doesn’t mention – they often carry the most actionable signal.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Basophil levels and immune health require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.