
Iron Blood Test: The Performance Mineral Your Doctor Is Measuring Wrong
You get your blood panel back. Iron is “normal.” Your doctor says nothing. You move on, still exhausted, still struggling through workouts that used to feel manageable, still hitting a mental wall by mid-afternoon.
Here’s the problem: standard iron testing is one of the most incomplete assessments in routine medicine. A single serum iron reading tells you almost nothing about your actual iron status. Without ferritin, transferrin saturation, TIBC, and the full iron panel in context, “normal iron” is a meaningless statement, and millions of people are walking around with functionally impaired iron status that never gets caught because the right questions aren’t being asked.
Iron is the mineral at the center of oxygen transport, energy production, cognitive function, immune defense, and thyroid metabolism. When iron status is suboptimal, not just clinically deficient, but below the threshold needed for peak biological function, the performance consequences are real and measurable. Fatigue that doesn’t resolve with sleep. Exercise capacity that plateaus inexplicably. Brain fog that coffee can’t fix. Cold intolerance. Hair that thins. Recovery that slows.
These aren’t vague complaints. They’re the predictable biological consequences of insufficient iron for optimal function, and they often appear well before hemoglobin drops enough to trigger an anemia diagnosis.
High performers don’t wait for clinical deficiency. They measure comprehensively, understand the full picture, and optimize iron status before it becomes a problem.
What Is Iron and What Does It Do?
Iron is an essential trace mineral, meaning your body cannot synthesize it and must obtain it entirely from dietary sources or supplementation. It’s the fourth most abundant element in the Earth’s crust, but inside the human body, it’s precious, tightly regulated, and absolutely essential for life.
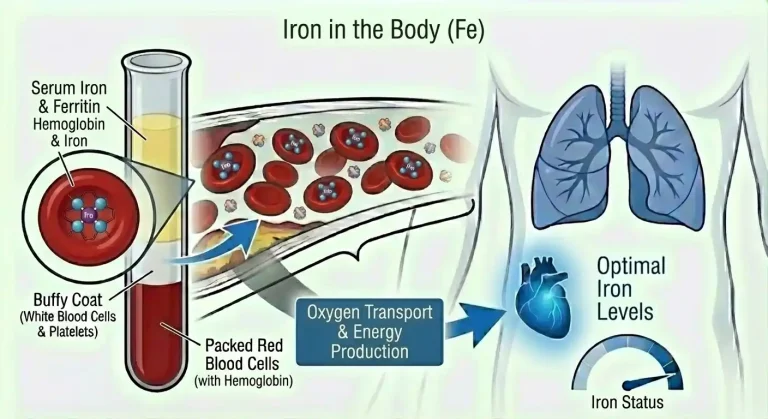
Iron’s central role is in oxygen transport. As a core component of hemoglobin, the protein in red blood cells that carries oxygen from lungs to tissues, iron is the functional heart of your oxygen delivery system. Each hemoglobin molecule contains four iron atoms, each capable of binding one oxygen molecule. Without adequate iron, hemoglobin production falls, red blood cells carry less oxygen, and every tissue in your body operates under conditions of relative oxygen deprivation.
But iron’s role extends far beyond oxygen transport. Iron is required for myoglobin, the oxygen-storing protein in muscle tissue that provides oxygen directly to muscle cells during exercise, enabling sustained muscular contraction. It’s a cofactor for cytochrome enzymes in the mitochondrial electron transport chain, the biological machinery that converts nutrients into ATP, the energy currency that powers every cellular process. Iron is essential for the synthesis of neurotransmitters including dopamine, serotonin, and norepinephrine, which explains why iron deficiency so consistently impairs mood and cognitive function. It’s required for DNA synthesis and cell division, meaning rapidly proliferating cells are particularly vulnerable to iron insufficiency. It’s critical for thyroid hormone metabolism, immune cell function, and collagen synthesis.
Iron exists in your body in several forms serving different functions. Functional iron is iron actively doing a job, primarily in hemoglobin (about 65-70% of total body iron), myoglobin (about 10%), and enzymes. Storage iron sits in reserve as ferritin and hemosiderin, primarily in the liver, spleen, and bone marrow, available to be mobilized when functional iron demands increase. Transport iron is iron in transit, bound to the protein transferrin and circulating in plasma on its way to where it’s needed.
The form your body uses depends entirely on availability and demand, a sophisticated regulatory system governed primarily by the hormone hepcidin, produced in the liver, which acts as iron’s master regulator.
Iron comes in two dietary forms with dramatically different bioavailability. Heme iron comes from animal sources, red meat, organ meats, poultry, and seafood. It’s directly absorbed by intestinal cells through a dedicated receptor and has absorption rates of 15-35% regardless of the body’s iron status. Non-heme iron comes from plant sources, legumes, leafy greens, fortified grains, nuts, seeds. Its absorption is highly variable (2-20%) and heavily influenced by enhancers like vitamin C and inhibitors like phytates, oxalates, calcium, and polyphenols. The practical implication is that dietary iron quality matters enormously, not just quantity, and people relying primarily on plant sources to meet iron needs are working significantly harder to achieve the same result.
Why Iron Matters for Performance and Health
Iron’s impact on performance is both direct and pervasive, touching virtually every system involved in how you feel, think, and physically perform.
Oxygen delivery and exercise capacity are the most direct connections. Iron determines hemoglobin, hemoglobin determines oxygen-carrying capacity, and oxygen-carrying capacity determines how much work your muscles and brain can sustain. Iron-deficient individuals, even before anemia develops, show measurably reduced VO2 max, earlier lactate threshold, greater perceived exertion at the same workload, and slower recovery. Competitive endurance athletes understand this intuitively, iron status is one of the most closely monitored variables in elite training because even minor depletion of iron stores produces meaningful performance decrements.
Energy production at the cellular level is impaired by iron deficiency independently of oxygen delivery. Iron-containing cytochrome enzymes in the mitochondrial electron transport chain are required for aerobic ATP synthesis. When these enzymes are iron-limited, mitochondrial energy production is compromised even when oxygen is technically available. People with iron deficiency experience this as fatigue that goes beyond what reduced oxygen delivery alone explains, a cellular energy deficit that affects every tissue simultaneously.
Cognitive function and mental performance are highly sensitive to iron status. The brain is one of the most metabolically demanding organs in the body, consuming roughly 20% of total oxygen supply. Beyond oxygen dependence, iron is directly required for the synthesis of dopamine, serotonin, and norepinephrine, the neurotransmitters that govern motivation, focus, mood regulation, and executive function. Iron deficiency, even without anemia, consistently produces measurable impairments in attention, working memory, information processing speed, and executive function. The performance-focused person experiencing inexplicable brain fog, reduced motivation, or difficulty sustaining concentration should have iron status at the top of their investigation list.
Thyroid function is directly linked to iron status in a relationship that’s frequently overlooked. Iron is a cofactor for thyroid peroxidase, the enzyme responsible for synthesizing thyroid hormones T3 and T4. Iron deficiency impairs thyroid hormone production and reduces the conversion of T4 to the more active T3. This creates a state of functional hypothyroidism even when thyroid markers appear technically normal, fatigue, cold intolerance, slowed metabolism, difficulty with weight management, and brain fog that looks exactly like thyroid disease but originates in iron insufficiency.
Immune function depends critically on iron. Iron is required for the proliferation and differentiation of immune cells, lymphocytes, neutrophils, and macrophages all have high iron demands during immune activation. Iron deficiency impairs both innate and adaptive immune responses, reducing the ability to fight infections effectively and slowing recovery from illness.
Hair, skin, and connective tissue health reflect iron status visibly. Iron is required for collagen synthesis, which provides structural integrity to skin, hair follicles, and connective tissue. Iron deficiency is one of the most common reversible causes of hair loss, specifically the diffuse thinning pattern called telogen effluvium, where hair prematurely enters the shedding phase. Many people pursuing hair loss treatments overlook iron status entirely, missing the most straightforward intervention available.
The Iron Biomarkers That Actually Matter
This is where standard medicine consistently fails people. A single serum iron reading without the surrounding markers is like checking one cylinder of a car engine and declaring it healthy. Iron status requires a panel of markers interpreted together.
Serum iron measures the amount of iron currently circulating in plasma, bound to transferrin. It reflects your current iron availability snapshot, and it’s the most misleading marker in isolation. Serum iron fluctuates dramatically throughout the day (levels can vary 30-50% from morning to afternoon), is affected by recent dietary intake, rises temporarily during infections and inflammatory states due to hepcidin regulation, and can appear normal even when iron stores are severely depleted. A single serum iron reading without context is nearly meaningless for assessing true iron status.
Ferritin is the single most important iron marker for assessing iron status in most people. Ferritin is the protein that stores iron in cells, primarily in the liver, spleen, and bone marrow, and a small amount circulates in blood, providing an indirect but reliable estimate of total body iron stores. This is the marker that standard medicine consistently misinterprets.
The reference range for ferritin extends as low as 12-15 ng/mL in many laboratories, technically “not deficient” but functionally catastrophic from a performance standpoint. Research consistently shows that iron deficiency symptoms, fatigue, reduced exercise capacity, impaired cognitive function, hair loss, appear at ferritin levels below 30-50 ng/mL, well above the clinical deficiency threshold.
Optimal ferritin for performance is considerably higher than the clinical minimum. Most research on non-anemic iron deficiency and functional performance supports ferritin targets of 50-100 ng/mL for baseline health, with many sports medicine and performance medicine practitioners targeting 70-150 ng/mL for athletes and highly active individuals.
The nuance on ferritin: it’s also an acute phase reactant, meaning it rises with inflammation, infection, and liver disease independently of iron stores. Someone with significant chronic inflammation can have ferritin of 60 ng/mL and still have depleted iron stores, because inflammatory signals drive ferritin production artificially. Interpreting ferritin alongside hs-CRP helps distinguish true iron repletion from inflammation-driven elevation.
Transferrin and TIBC (total iron binding capacity) measure the iron transport system. Transferrin is the protein that carries iron through the bloodstream. TIBC measures the total capacity of transferrin to bind iron. In iron deficiency, transferrin production increases (the body upregulates transport capacity trying to capture more iron), so TIBC rises while serum iron falls. In iron overload, TIBC decreases as binding sites are saturated. TIBC rising while serum iron falls is a classic pattern of iron deficiency even when ferritin is borderline.
Transferrin saturation (TSAT) is calculated by dividing serum iron by TIBC and expressing it as a percentage, it tells you what fraction of available transferrin is actually carrying iron. Optimal transferrin saturation is 20-45%. Below 20% indicates insufficient iron supply relative to transport capacity, pointing toward functional iron deficiency. Above 45% suggests iron loading or excess. TSAT below 20% alongside low ferritin is strong corroborating evidence of iron deficiency. TSAT below 20% with normal or high ferritin can indicate functional iron deficiency driven by inflammation (iron is stored but not being released effectively).
Hemoglobin and hematocrit reflect the downstream consequence of iron status on red blood cell production. These are the last markers to change in iron deficiency, hemoglobin only drops once iron stores are severely depleted and hemoglobin synthesis is directly impaired. Using hemoglobin as your primary iron assessment tool means you won’t catch iron deficiency until it’s advanced enough to cause anemia. This is exactly the mistake standard medicine makes.
Reticulocytes are immature red blood cells newly released from bone marrow. Reticulocyte count and reticulocyte hemoglobin content (CHr or Ret-He) reflect whether the bone marrow is producing adequately hemoglobinized new cells, a sensitive early indicator of functional iron deficiency even before ferritin or hemoglobin show clear abnormalities.
The sequence of iron depletion matters for understanding your results. First, ferritin falls as iron stores deplete. Then, serum iron falls and TIBC rises as stores become insufficient to maintain normal transport. Then, transferrin saturation drops as less iron is available for transport. Then, hemoglobin production falls and anemia develops. Most routine blood tests only catch iron deficiency at the final stage. Comprehensive iron assessment catches it at the first.
Normal vs. Optimal Iron Markers
Standard reference ranges versus performance-optimized targets reveal a significant gap.
Ferritin: Standard “normal” lower limit: 12-15 ng/mL (women), 30 ng/mL (men) Optimal for performance: 70-150 ng/mL (men and women) Optimal for active individuals and athletes: 100-150 ng/mL
Serum iron: Standard reference range: 60-170 mcg/dL Optimal: 80-150 mcg/dL (context-dependent alongside other markers)
TIBC: Standard reference range: 250-370 mcg/dL Elevated TIBC (above 370) suggests iron deficiency; reduced TIBC suggests iron excess or chronic disease
Transferrin saturation: Standard reference range: 15-50% Optimal: 25-40% Below 20% with low-normal ferritin indicates functional deficiency
Hemoglobin: Standard “normal” lower limit: 13.5 g/dL (men), 12.0 g/dL (women) Optimal: 15.0-17.0 g/dL (men), 14.0-16.0 g/dL (women) (See hemoglobin biomarker page for full discussion)
The pattern matters more than any individual number. Low-normal ferritin with low-normal transferrin saturation and low-normal serum iron tells a clear story of suboptimal iron status even when every individual marker technically falls within the reference range. This is exactly the scenario where standard interpretation fails and comprehensive assessment reveals what’s actually happening.
What Causes Iron Deficiency?
Iron deficiency develops through three primary mechanisms, inadequate intake, impaired absorption, and excess loss, often in combination.
Inadequate dietary intake is common across several populations. Plant-based and vegan diets eliminate heme iron entirely, relying solely on non-heme iron with its inherently lower and more variable bioavailability. People following restrictive diets for weight loss or food sensitivity management often inadvertently reduce iron intake. Athletes, particularly endurance athletes, have dramatically elevated iron requirements due to increased red blood cell turnover, iron losses through sweat, and gastrointestinal microbleeding from high training volumes, meaning standard intake recommendations are often insufficient.
Impaired absorption is underappreciated and frequently missed. Celiac disease damages the intestinal villi where iron absorption occurs, producing profound iron deficiency that persists until gluten is eliminated. H. pylori infection impairs gastric acid production, which is required to reduce dietary iron to its absorbable form, treating H. pylori often normalizes iron absorption without any iron supplementation. Atrophic gastritis and proton pump inhibitor (PPI) use both reduce gastric acid, impairing iron absorption over time. Inflammatory bowel disease affects both absorption and blood loss. Even without a diagnosable condition, some individuals simply have constitutionally lower iron absorption efficiency that requires higher dietary intake or supplementation to maintain adequate stores.
Dietary inhibitors of iron absorption compound the problem for many people. Calcium competes directly with iron for absorption, consuming dairy, calcium supplements, or calcium-fortified foods alongside iron-rich meals significantly reduces iron uptake. Coffee and tea contain polyphenols that bind non-heme iron and reduce absorption by 50-90% when consumed with meals. Phytates in whole grains and legumes bind iron and reduce its bioavailability. These aren’t reasons to avoid these foods, but consuming them strategically, separated from iron-rich meals and supplementation, meaningfully improves iron absorption.
Blood loss is the most common cause of iron deficiency in otherwise healthy individuals with adequate dietary intake. Menstruation is the primary culprit in premenopausal women, monthly blood loss of 30-80 mL depletes iron stores progressively without adequate dietary replacement. Women with heavy menstrual bleeding lose substantially more, making iron deficiency nearly inevitable without targeted supplementation. Gastrointestinal blood loss from any source, ulcers, gastritis, polyps, inflammatory bowel disease, hemorrhoids, colorectal cancer, produces chronic iron depletion that may not be immediately apparent. Unexplained iron deficiency in men or postmenopausal women should always prompt gastrointestinal evaluation to rule out occult bleeding. Frequent blood donation depletes iron stores, regular donors who give more than 2-3 times per year commonly develop progressively lower ferritin.
Functional iron deficiency from chronic inflammation is a distinct mechanism where total body iron may be adequate but iron is locked away in storage and unavailable for use. Hepcidin, the master iron regulator, rises in response to inflammation and infection, blocking iron release from storage cells and reducing intestinal iron absorption. People with chronic inflammatory conditions, obesity-related inflammation, or chronic infections can have seemingly normal or even elevated ferritin (because ferritin is an acute phase reactant) while having functionally impaired iron availability for hemoglobin synthesis and cellular processes. This is why ferritin context matters, a ferritin of 60 ng/mL with significant inflammation may represent functional iron deficiency, while the same ferritin in a healthy, non-inflamed individual reflects adequate stores.
Intense exercise creates iron demands that exceed what most active people account for. Distance running causes intravascular hemolysis, the mechanical destruction of red blood cells from foot-strike impact with hard surfaces, releasing hemoglobin into plasma that is then cleared renally, depleting iron. High training volumes increase erythropoiesis (red blood cell production) demands, consuming iron stores rapidly. Exercise-induced inflammatory responses temporarily elevate hepcidin, reducing iron absorption in the hours following intense training. Elite endurance athletes often require iron intakes far exceeding standard recommendations and benefit from regular iron status monitoring to maintain ferritin at levels supporting peak performance.
What Causes Iron Excess?
While iron deficiency dominates the clinical conversation, iron excess, iron overload, is equally serious and more common than most people realize.
Hereditary hemochromatosis is the most common serious genetic condition in populations of Northern European descent, affecting approximately 1 in 200-300 individuals. Mutations in the HFE gene cause the body to absorb iron excessively from the diet, progressively loading iron into organs, primarily the liver, heart, pancreas, and joints, causing progressive damage over decades. Many people with hemochromatosis are undiagnosed until organ damage has accumulated substantially. Elevated transferrin saturation (above 45-50%) combined with elevated ferritin should prompt HFE genetic testing.
Chronic liver disease impairs the liver’s role in iron regulation and can produce secondary iron overload. Alcoholic liver disease and non-alcoholic fatty liver disease both alter iron metabolism.
Excessive supplementation, taking high-dose iron supplements without confirmed deficiency or medical guidance, can progressively elevate iron stores. Iron is not water-soluble and is not easily excreted, the body has limited mechanisms for eliminating excess iron, which is why iron overload accumulates insidiously.
Multiple blood transfusions deliver substantial iron with each unit of packed red blood cells, producing iron loading in people requiring frequent transfusions.
The risks of iron overload are serious and distinct from iron deficiency. Excess iron is a pro-oxidant, it catalyzes free radical production through Fenton chemistry, accelerating oxidative damage to cells and tissues. Iron overload causes liver fibrosis and cirrhosis, diabetes from pancreatic iron loading (bronze diabetes), cardiomyopathy and heart failure, arthropathy and joint damage, skin bronzing, and significantly increased cancer risk. Elevated iron is also associated with increased risk of infections because iron is required by pathogens, iron overload creates a favorable environment for bacterial and fungal growth.
This is why iron supplementation should never be undertaken without confirmed deficiency, and why testing ferritin and transferrin saturation is essential before beginning any iron supplementation protocol.
How to Optimize Iron Status
Iron optimization requires a nuanced approach, getting enough without getting too much, addressing the root causes of deficiency, and optimizing absorption rather than just increasing intake.
Maximize dietary iron quality and bioavailability. Prioritize heme iron from red meat, organ meats (liver is extraordinarily iron-dense), dark poultry meat, and shellfish, particularly oysters and clams. These provide the most bioavailable iron with the least absorption variability. Include non-heme iron sources, lentils, white beans, tofu, pumpkin seeds, dark leafy greens, but pair them with vitamin C-rich foods (citrus, bell peppers, strawberries, broccoli) to meaningfully enhance absorption.
Separate iron-rich meals from absorption inhibitors. Consume coffee, tea, calcium-rich foods, and calcium supplements at different times than your primary iron sources. This simple timing adjustment can double or triple iron absorption from the same dietary intake without changing what you eat.
Supplement strategically when diet is insufficient. When ferritin is below 50 ng/mL and dietary optimization isn’t closing the gap, iron supplementation is appropriate. Standard supplemental doses range from 25-65 mg elemental iron daily, the actual elemental iron content varies by iron salt form (ferrous sulfate is most commonly used but ferrous bisglycinate is often better tolerated). Take supplemental iron with vitamin C and away from meals containing absorption inhibitors. Every other day dosing has emerging evidence for better net absorption and fewer GI side effects than daily dosing, because daily supplementation triggers temporary hepcidin elevation that reduces absorption of the next day’s dose.
Monitor ferritin every 2-3 months during supplementation to confirm repletion and avoid overloading. Stop supplementing once ferritin reaches the target range of 70-150 ng/mL and maintain through diet.
Address root causes of poor absorption. Test for H. pylori if iron deficiency is unexplained, treatment often resolves absorption problems. Evaluate for celiac disease if iron deficiency persists despite adequate intake and supplementation. Review all medications that may impair iron absorption, PPIs, antacids, certain antibiotics, and others. Consider gastric acid support (digestive enzymes, betaine HCl under physician guidance) if low stomach acid is suspected.
Manage blood loss sources. For women with heavy menstrual bleeding, discuss management options with a gynecologist, hormonal interventions that reduce menstrual blood loss often resolve iron deficiency without requiring lifelong supplementation. For anyone with unexplained iron deficiency, particularly men or postmenopausal women, gastrointestinal evaluation to rule out occult bleeding is essential before assuming dietary insufficiency.
Reduce chronic inflammation to improve functional iron availability. When hepcidin is chronically elevated due to inflammatory conditions, iron absorption and release from stores is impaired regardless of total body iron content. Addressing the inflammatory driver, whether metabolic, infectious, or autoimmune, normalizes hepcidin and improves functional iron utilization.
For athletes and highly active individuals, iron monitoring should be routine, ideally every 3-6 months including ferritin, serum iron, and transferrin saturation alongside hemoglobin. Running athletes in particular should evaluate iron status whenever unexplained performance decrements occur.
Iron and Metabolic Health
The relationship between iron and metabolic function runs deeper than most people appreciate.
Iron is required for optimal thyroid function, as a cofactor for thyroid peroxidase enzyme that synthesizes thyroid hormones. Iron deficiency produces measurable impairment in thyroid hormone synthesis and T4-to-T3 conversion, creating functional hypothyroid states that respond to iron repletion rather than thyroid hormone replacement. People diagnosed with subclinical hypothyroidism or experiencing hypothyroid symptoms should have comprehensive iron status assessed before defaulting to thyroid medication.
Iron overload creates distinct metabolic problems. Excess iron in the pancreas impairs insulin secretion, contributing to glucose dysregulation and diabetes risk. Iron overload in the liver promotes hepatic insulin resistance and fatty liver disease. Addressing iron overload through therapeutic phlebotomy often improves metabolic markers substantially.
Hepcidin, the master iron regulator, is elevated by both inflammation and insulin resistance, creating functional iron deficiency in metabolically unhealthy individuals despite potentially adequate iron stores. Improving metabolic health, particularly reducing insulin resistance, normalizes hepcidin and improves iron availability.
Iron and Hormone Optimization
Iron intersects with hormonal health in several important ways that matter for performance-focused individuals.
Testosterone optimization is directly relevant to iron status. Testosterone stimulates erythropoiesis, red blood cell production, which increases iron demand. Men initiating testosterone replacement therapy often see hemoglobin and hematocrit rise substantially, which increases iron consumption. Iron status should be assessed before and during testosterone therapy, and ferritin monitored to ensure iron stores support the increased erythropoietic demand.
Conversely, men on testosterone therapy who develop elevated hematocrit (above 52-54%) may require therapeutic phlebotomy to reduce red blood cell mass, which also depletes iron stores, requiring careful monitoring to avoid inducing deficiency.
For women, the intersection of iron status and hormonal health is even more direct. Estrogen influences iron metabolism, and estrogen decline in perimenopause and menopause, alongside cessation of menstrual blood loss, dramatically changes iron balance. Postmenopausal women often see ferritin rise substantially compared to their premenopausal baseline. The same woman who required iron supplementation throughout her reproductive years may develop iron excess in menopause without any change in diet or supplementation. Iron status assessment should be part of routine hormonal health monitoring in perimenopause and beyond.
Frequently Asked Questions
What are the symptoms of low iron?
Symptoms of suboptimal iron status, even without clinical anemia, include persistent fatigue that doesn’t resolve with adequate sleep, reduced exercise capacity and earlier onset of exhaustion during physical activity, brain fog and difficulty concentrating, impaired memory and processing speed, low mood and reduced motivation, cold intolerance, hair thinning or increased shedding, brittle nails, pale skin, shortness of breath with exertion, headaches, and restless legs syndrome. These symptoms often appear when ferritin falls below 30-50 ng/mL, well before hemoglobin drops enough to diagnose anemia.
Is it possible to have iron deficiency with normal hemoglobin?
Absolutely, and this is the most common scenario that standard medicine misses. Iron depletion follows a predictable sequence: ferritin falls first, then serum iron and transferrin saturation decline, and only finally does hemoglobin drop into anemic range. The symptomatic phase of iron deficiency, where performance, cognitive function, and energy are impaired, typically occurs during the ferritin-depleted, normal-hemoglobin phase. This is why ferritin is the critical marker, not hemoglobin.
How much iron do I need daily?
Dietary reference intakes for iron are 8 mg/day for adult men and postmenopausal women, 18 mg/day for premenopausal women, and 27 mg/day during pregnancy. But these are minimums to prevent deficiency in average sedentary individuals, not targets for performance optimization. Endurance athletes, particularly runners, may have iron requirements 70-100% higher than sedentary recommendations. People with poor absorption efficiency, heavy menstrual losses, or active iron depletion require substantially more. Individual needs vary considerably, which is why testing rather than estimating is the appropriate strategy.
What foods are highest in iron?
Organ meats lead the list, beef liver contains roughly 6 mg iron per 100g, mostly as highly bioavailable heme iron. Oysters and clams are exceptionally iron-dense shellfish, providing 5-8 mg per serving. Red meat (beef, lamb) provides 2-3 mg per 100g as heme iron. Dark poultry meat provides 1-2 mg. Among plant sources, white beans, lentils, and tofu provide 3-4 mg per serving as non-heme iron, but absorption is highly variable. Pumpkin seeds, dark chocolate, and fortified cereals contribute non-heme iron but with lower effective delivery.
Can I take iron supplements every day?
Current evidence suggests that alternate-day dosing, supplementing every other day rather than daily, produces better net iron absorption than daily dosing for most people. Daily iron supplementation causes hepcidin to rise the following day, reducing absorption of the next dose. Alternate-day dosing allows hepcidin to normalize between doses, improving total iron absorbed per milligram ingested. It also tends to produce fewer gastrointestinal side effects. That said, supplementation protocol should be guided by your individual iron status, severity of deficiency, and physician guidance.
What’s the difference between ferrous sulfate and ferrous bisglycinate?
Both are common supplemental iron forms. Ferrous sulfate is more widely studied and less expensive but produces more gastrointestinal side effects (constipation, nausea, stomach discomfort) because unabsorbed iron in the gut is irritating. Ferrous bisglycinate (iron chelated to the amino acid glycine) is better absorbed, requires lower doses to achieve the same iron delivery, and produces significantly fewer GI side effects. For people who struggle to tolerate standard iron supplements, ferrous bisglycinate is generally the preferred alternative.
How long does it take to raise ferritin?
With appropriate supplementation, ferritin typically begins rising within 4-6 weeks. However, fully repleting depleted iron stores takes considerably longer, 3-6 months of consistent supplementation is typical to bring ferritin from deficient levels (below 20 ng/mL) to the optimal range (70-150 ng/mL). Hemoglobin responds faster, typically 2-4 weeks if anemia was present. The mistake most people make is stopping supplementation once hemoglobin normalizes, leaving ferritin still depleted and stores unreplenished.
Is iron from red meat bad for heart health?
The relationship between dietary iron intake, particularly heme iron from red meat, and cardiovascular risk is more nuanced than headlines suggest. Heme iron from unprocessed red meat has a much weaker association with cardiovascular outcomes than heme iron from processed meats (bacon, hot dogs, cured deli meats), which contain additional confounding factors. For people without hereditary hemochromatosis or iron overload, consuming moderate amounts of unprocessed red meat as an iron source poses minimal cardiovascular risk in the context of an otherwise healthy diet. Monitoring iron markers, particularly ferritin and transferrin saturation, ensures you’re not accumulating excess iron regardless of dietary source.
Testing Iron With ApexBlood
ApexBlood’s comprehensive blood panel includes the full iron assessment that actually tells you where you stand, ferritin, serum iron, TIBC, and transferrin saturation alongside hemoglobin, hematocrit, and the complete blood count. This is the only way to interpret iron status correctly, not a single number in isolation, but the full picture of iron stores, transport, utilization, and downstream effects.
Understanding whether fatigue, reduced performance, or brain fog reflects iron insufficiency requires looking at all of these markers together, alongside the metabolic, hormonal, and inflammatory context that influences iron regulation. A ferritin of 45 ng/mL means something very different in an inflamed, metabolically unhealthy person than it does in a lean, low-inflammation individual. Context is everything, and comprehensive testing provides it.
Most physicians check hemoglobin and call it an iron assessment. It isn’t. High performers understand that catching iron insufficiency in the ferritin-depletion phase, before hemoglobin falls, before performance has significantly declined, is where the real value of comprehensive testing lives.
Get comprehensive testing, $189
The Bottom Line on Iron
Iron is the mineral at the foundation of oxygen transport, cellular energy production, cognitive function, thyroid metabolism, and immune defense. When iron status is suboptimal, not just clinically deficient, but below the threshold required for peak biological function, the performance consequences show up in every system simultaneously.
The problem isn’t that iron deficiency is rare. It’s that it’s routinely missed because the right markers aren’t being assessed. Checking hemoglobin alone catches iron deficiency only after it’s advanced to anemia. Checking ferritin, transferrin saturation, TIBC, and serum iron together catches it in the functionally impaired phase, when intervention is straightforward and the performance return is substantial.
Optimal ferritin for performance is 70-150 ng/mL, not the 12-15 ng/mL floor that standard labs consider acceptable. Optimal transferrin saturation is 25-40%. Optimal hemoglobin is 15.0-17.0 g/dL for men and 14.0-16.0 g/dL for women. These targets reflect what your biology needs to function at its best, not what it needs to avoid a clinical diagnosis.
Iron optimization means eating strategically for bioavailability, addressing root causes of poor absorption or excess loss, supplementing when needed with appropriate monitoring, and avoiding the equally serious problem of iron overload that occurs when supplementation proceeds without testing.
High performers don’t wait for anemia to address iron status. They measure comprehensively, interpret correctly, and act on what the data shows, because the difference between depleted iron stores and optimized iron status is the difference between operating below your biological potential and operating at it.
You can’t optimize what you don’t measure. Stop accepting incomplete iron assessment when comprehensive testing reveals what a single number never can.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Iron status and related conditions require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.