
Basophils are the rarest of the five white blood cell types, typically making up less than 1% of your circulating white blood cells. Because they are so scarce, many people assume they are unimportant – but basophils play a highly specialized role in allergic responses, inflammation, and immune system modulation that makes them worth understanding. An elevated basophil count (basophilia) is one of the few white blood cell abnormalities that should prompt investigation for specific conditions including myeloproliferative disorders and systemic inflammatory states. An extremely low or absent basophil count can also carry clinical significance. For anyone using comprehensive blood panels to monitor health and optimize immune function, understanding basophils – what they do, what drives them up or down, and when abnormalities warrant follow-up – completes the picture of immune health surveillance.
What Are Basophils?
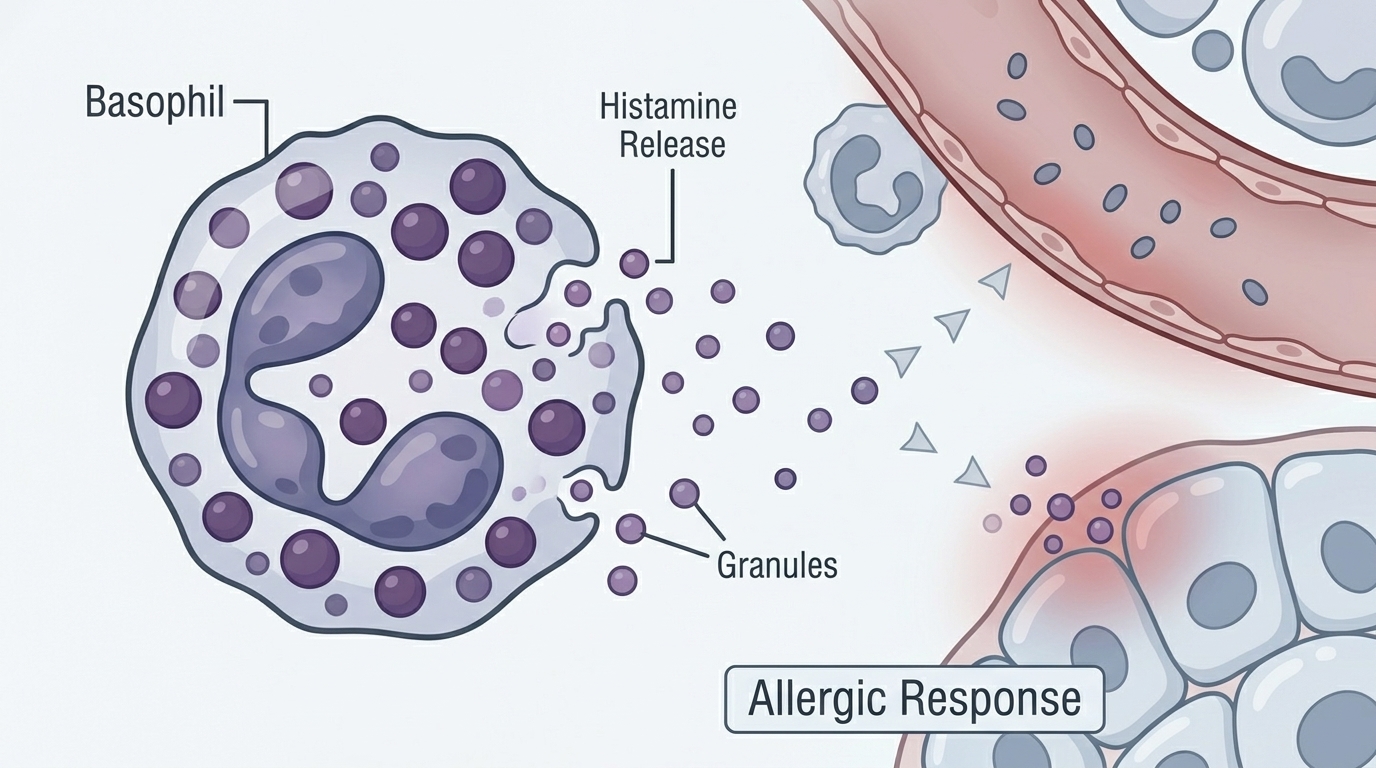
Basophils are granulocytes – white blood cells containing granules filled with biologically active compounds – that are produced in the bone marrow from the same myeloid progenitor cells as other granulocytes (neutrophils and eosinophils). The name “basophil” comes from the fact that these cells stain strongly with basic dyes in laboratory preparations, producing a characteristic dark blue/purple granular appearance under the microscope. This staining reflects the highly charged, sulfated contents of the granules.
Basophil granules contain a potent mixture of inflammatory mediators: histamine (the primary driver of allergic symptoms), heparin (a natural anticoagulant), leukotrienes, prostaglandins, and various cytokines including IL-4 and IL-13. When basophils are activated by allergen exposure (via IgE antibodies bound to basophil surface receptors) or by complement proteins, they degranulate – rapidly releasing these contents into the surrounding tissue. This causes the classic features of immediate allergic responses: vasodilation, increased vascular permeability, smooth muscle contraction, mucus secretion, and recruitment of additional immune cells.
Why Basophils Matter for Immune Health Monitoring
For most healthy adults, basophil counts remain low and stable. But basophil count abnormalities carry diagnostic significance that makes them worth tracking in comprehensive health panels. Basophilia – elevated basophil counts – is relatively uncommon in routine blood work, which means when it is present, it is more likely to indicate a real underlying process. The most important conditions associated with persistent basophilia include myeloproliferative neoplasms (particularly chronic myelogenous leukemia, polycythemia vera, and essential thrombocythemia), which are bone marrow diseases that cause overproduction of multiple blood cell lines including basophils.
Beyond serious hematologic conditions, basophilia can reflect active allergic disease, inflammatory conditions, and certain infections – providing a signal that systemic inflammation or immune activation is present even before other symptoms become obvious. For health optimizers monitoring immune function longitudinally, a rising basophil count on serial panels is a finding that warrants investigation rather than reassurance.
Normal vs. Optimal Basophil Levels
Standard Reference Ranges: Basophils are reported as a percentage of total white blood cells (typically 0-1%) and as an absolute count (typically 0-0.1 x10³/µL or 0-100 cells/µL). Because basophils are normally so rare, even a small change in absolute count can translate to a large percentage change – a basophil count of 0.15 x10³/µL might be reported as 1.5%, slightly above the reference range. Most adults have basophil counts below 0.05 x10³/µL at any given time.
The Problem With “Normal”: Basophils circulate in very small numbers that fluctuate based on time of day, immune activation state, and stress. A single slightly elevated basophil count should be confirmed on repeat testing before drawing conclusions. The key question with any basophilia is whether it is transient and reactive (from allergy, inflammation, or infection) or persistent (suggesting a primary bone marrow process). A single measurement provides limited information; trends over time are more meaningful.
Optimal Basophil Count: For healthy adults without active allergic disease or inflammation, basophil counts are typically very low – often 0-0.05 x10³/µL. Counts in this range with normal other CBC parameters and no symptoms are reassuring. The focus with basophils is not on optimization in the way energy or performance markers are optimized, but on identification of persistent abnormalities that warrant investigation.
What Causes High Basophils (Basophilia)?
Myeloproliferative neoplasms are the most clinically significant cause of persistent basophilia. Chronic myelogenous leukemia (CML) – a cancer driven by the BCR-ABL fusion gene – reliably causes basophilia and is one of the rare situations where an elevated basophil count is specifically diagnostic in the right clinical context. Polycythemia vera (overproduction of red blood cells), essential thrombocythemia (overproduction of platelets), and myelofibrosis also cause basophilia as part of general bone marrow overproduction. Any unexplained persistent basophilia above 0.1 x10³/µL warrants hematology consultation.
Reactive causes of basophilia include allergic and atopic diseases (asthma, eczema, hay fever, food allergies), hypothyroidism (thyroid hormone normally suppresses basophil production), inflammatory bowel disease, rheumatoid arthritis and other autoimmune conditions, certain infections (particularly viral), and iron deficiency. Basophilia from reactive causes is typically mild (0.1-0.2 x10³/µL) and transient, resolving when the underlying condition is treated.
What Causes Low Basophils (Basopenia)?
Because basophils are normally so rare, a count near zero is not inherently abnormal. True basopenia (clinically significant absence of basophils) is relatively uncommon but can occur with acute severe allergic reactions (basophils degranulate and temporarily disappear from circulation), hyperthyroidism (thyroid hormone suppresses basophil count), acute corticosteroid use (steroids suppress basophils as part of their anti-inflammatory effect), and during acute infections with severe immune activation. Prolonged basopenia can occasionally be a sign of underlying bone marrow suppression, though this would typically be accompanied by abnormalities in other blood cell lines.
Frequently Asked Questions
Should I be worried if my basophil count is slightly elevated?
A single slightly elevated basophil count (0.1-0.15 x10³/µL) is often reactive – from allergies, mild inflammation, or normal biological variation. The critical question is whether the elevation is persistent. If basophil counts are elevated on multiple blood panels over months, or if the elevation is significant (above 0.2 x10³/µL), or if other blood cell lines are also abnormal, this warrants hematology consultation to rule out myeloproliferative disease. A single mildly elevated basophil count in otherwise normal blood work can reasonably be rechecked in 2-3 months.
Is there a connection between basophils and allergies?
Yes, directly. Basophils express high-affinity IgE receptors (FcεRI) on their surface. When you are sensitized to an allergen (dust mites, pollen, certain foods, insect venom), IgE antibodies specific to that allergen bind to these surface receptors. The next time you encounter the allergen, it cross-links these IgE-receptor complexes and triggers basophil degranulation – the rapid release of histamine and other inflammatory mediators that produce allergic symptoms. This is essentially the same mechanism as mast cell degranulation in tissues. People with active allergic disease often have mildly elevated basophil counts and more reactive basophils on functional testing.
What is the difference between basophils and mast cells?
Basophils and mast cells share many characteristics – both express IgE receptors, both contain histamine-rich granules, both respond to allergen exposure and complement activation – but they are distinct cell types with important differences. Basophils circulate in the blood and can be counted on a CBC. Mast cells reside in tissues (skin, mucosa, connective tissue) and are not visible on a standard blood count. Mast cells are longer-lived and more proliferative in tissues than basophils. Both cell types contribute to allergic responses, but mast cells are the primary effectors in tissue (the immediate wheal-and-flare reaction to a skin prick test), while basophils contribute more to systemic and late-phase allergic reactions.
Can stress affect basophil counts?
Yes. Physiological and psychological stress activates the hypothalamic-pituitary-adrenal (HPA) axis, increasing cortisol. Cortisol suppresses basophil counts (along with eosinophils and lymphocytes) – this is a component of the acute stress response that shifts the immune system toward innate, rapid response rather than adaptive immune function. Sustained high-stress states with chronically elevated cortisol can suppress basophil counts. Conversely, resolution of chronic stress and normalization of HPA axis function may be associated with normalization of basophil and eosinophil counts if they were suppressed.
Testing Basophils With ApexBlood
Basophils are included in ApexBlood’s comprehensive CBC with differential, which provides the full white blood cell breakdown – neutrophils, lymphocytes, monocytes, eosinophils, and basophils – alongside red blood cell indices, platelets, and a complete metabolic panel. Our physicians review the complete CBC in context, not individual values in isolation, to identify patterns of immune activation, inflammation, or bone marrow abnormality that warrant follow-up.
Get comprehensive testing for $189
The Bottom Line on Basophils
Basophils are the immune system’s rare but specialized alarm cells – key mediators of allergic responses and important surveillance markers for bone marrow health. While a single mildly elevated basophil count is usually reactive and temporary, persistent basophilia is one of the more specific CBC abnormalities that warrants evaluation for myeloproliferative disease. Very low or absent basophils can reflect acute allergic responses, steroid use, or hyperthyroidism. The CBC differential is most powerful when interpreted as a complete immune profile rather than individual cell counts – and understanding what basophils specifically signal adds a layer of diagnostic precision to comprehensive blood monitoring. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Basophil counts and CBC results require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.