
Vitamin D is simultaneously one of the most important nutrients for human health and one of the most widespread deficiencies in the developed world. Despite decades of public health messaging about sun protection and reduced outdoor time, an estimated 40-50% of American adults are deficient or insufficient in vitamin D. More striking: the people who are most actively pursuing health – athletes, professionals with demanding indoor schedules, health-conscious individuals following conventional sun-avoidance guidance – are often among the most deficient. And while the clinical consequences of severe vitamin D deficiency are well-established (rickets, osteomalacia), the performance, immune, hormonal, and longevity implications of suboptimal vitamin D – technically “not deficient” but far from optimal – are where most people are losing ground they don’t even know they’ve lost.
What Is Vitamin D?
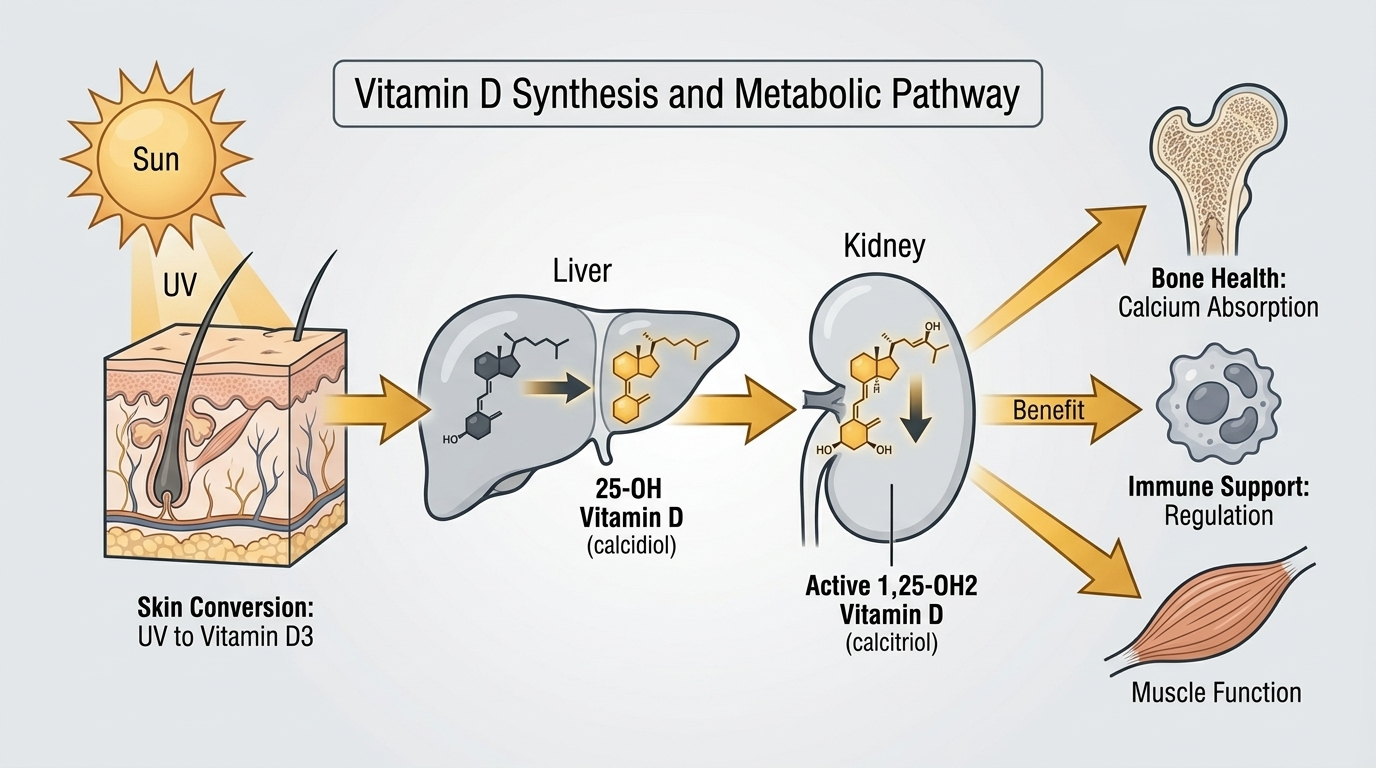
Despite being called a vitamin, vitamin D is more accurately classified as a prohormone – a precursor to a hormone that has widespread regulatory effects throughout the body. Vitamin D exists in two primary dietary forms: D2 (ergocalciferol, from plants and fungi) and D3 (cholecalciferol, from animal sources and produced in human skin). D3 is the more potent form and is what your body synthesizes from sunlight. Regardless of source, vitamin D undergoes a two-step activation process: first in the liver (converting to 25-hydroxyvitamin D, or 25(OH)D – the form measured in blood tests), and then in the kidneys and various tissues (converting to the active hormone 1,25-dihydroxyvitamin D, or calcitriol).
Vitamin D receptors (VDR) are present in virtually every tissue and cell type in the human body – immune cells, muscle cells, cardiac cells, neurons, pancreatic beta cells, and more. This ubiquity of receptors explains why vitamin D influences such a diverse range of biological processes beyond calcium metabolism: immune function, inflammation regulation, insulin sensitivity, muscle function, mood, cardiovascular health, and gene expression (calcitriol regulates approximately 200-2000 genes depending on the tissue). Vitamin D is not a single-purpose nutrient – it is a master regulatory signal with system-wide effects.
Why Vitamin D Matters for Performance, Immunity, and Longevity
The evidence base for vitamin D’s role in performance and longevity is extensive and growing. For athletes and active individuals, vitamin D is required for optimal muscle function – vitamin D receptors in skeletal muscle regulate protein synthesis, calcium handling, and force generation. Low vitamin D is associated with reduced muscle strength, higher injury rates (particularly stress fractures and muscle strains), impaired athletic recovery, and more frequent illness. Studies of athletes show that higher vitamin D levels correlate with better performance metrics across multiple sports, and that correcting deficiency improves strength, power output, and endurance.
For immune function, vitamin D is not just supportive – it is essential. Vitamin D activates antimicrobial peptides (cathelicidin, defensins) that are part of the innate immune defense against viruses and bacteria. It modulates adaptive immunity, reducing excessive inflammatory responses while supporting effective pathogen clearance. Vitamin D deficiency is associated with increased susceptibility to respiratory infections, longer illness duration, and higher rates of autoimmune disease. The relationship between vitamin D and COVID-19 severity was extensively studied during the pandemic, with multiple studies showing strong correlations between deficiency and poor outcomes.
For longevity, low vitamin D is associated with increased all-cause mortality, cardiovascular disease, Type 2 diabetes, multiple cancers (colorectal, breast, prostate), cognitive decline, depression, and autoimmune conditions. While causality versus correlation remains debated for some of these associations, the totality of evidence suggests that maintaining optimal vitamin D levels throughout life contributes meaningfully to healthspan and lifespan.
Normal vs. Optimal Vitamin D Levels
Standard Reference Ranges: Most laboratories define vitamin D sufficiency as 25(OH)D above 20 ng/mL (50 nmol/L), with deficiency below 12 ng/mL (30 nmol/L) and insufficiency between 12 and 20 ng/mL. The Institute of Medicine established these thresholds primarily based on bone health outcomes – the minimum vitamin D level needed to maintain normal calcium absorption and bone density. This bone-focused threshold captures only a fraction of vitamin D’s biological functions.
The Problem With “Normal”: A level of 21 ng/mL is technically “sufficient” by laboratory standards – but research consistently shows that vitamin D’s broader benefits (immune function, muscle performance, insulin sensitivity, mood, cancer protection) plateau at much higher levels. The Endocrine Society recommends 25-80 ng/mL as the optimal range. Leading longevity and functional medicine physicians typically target 50-70 ng/mL as the optimal range for comprehensive health benefits. Most Americans who are not supplementing fall in the 15-30 ng/mL range – sufficient to avoid bone disease but insufficient for optimal performance and immune function.
Optimal Vitamin D for Performance and Longevity: The evidence most consistently points to 40-70 ng/mL (100-175 nmol/L) as the target range for optimal health benefits beyond bone protection. Below 30 ng/mL, immune function, muscle performance, and inflammatory regulation are all suboptimal. Above 80-100 ng/mL, toxicity concerns begin to emerge (though true vitamin D toxicity is rare and typically requires supplementation at very high doses for prolonged periods). The goal for most adults is to supplement based on testing – not to a fixed arbitrary dose, but to achieve and maintain a measured level in the optimal range.
What Causes Low Vitamin D?
Inadequate sun exposure is the primary driver of widespread vitamin D deficiency in modern populations. Vitamin D synthesis requires UVB radiation (wavelengths 290-315 nm) to strike the skin and convert 7-dehydrocholesterol to pre-vitamin D3. This UVB radiation is only available at sufficient intensity when the sun is high in the sky – generally between 10 AM and 3 PM in summer months at latitudes below 35 degrees north. At higher latitudes (most of the United States north of Atlanta), UVB is insufficient for vitamin D synthesis for 4-6 months of the year. Consistent indoor work, sunscreen use, and sun-protective clothing all further reduce synthesis. Darker skin pigmentation (which evolved to protect against UV damage in high-sun environments) requires substantially more sun exposure to synthesize equivalent vitamin D – making darker-skinned individuals at particularly high risk of deficiency in northern latitudes.
Obesity reduces bioavailable vitamin D because vitamin D is fat-soluble and gets sequestered in adipose tissue, reducing circulating 25(OH)D levels proportionally to body fat percentage. Malabsorption from celiac disease, Crohn’s disease, cystic fibrosis, bariatric surgery, or other conditions impairing fat absorption reduces dietary vitamin D absorption. Kidney disease impairs the conversion of 25(OH)D to the active calcitriol form. Aging reduces skin synthesis capacity (by approximately 50% by age 70) and renal conversion efficiency. Certain medications (glucocorticoids, anticonvulsants, some HIV medications) accelerate vitamin D catabolism.
How to Optimize Vitamin D Levels
Supplementation is the most reliable method for achieving and maintaining optimal vitamin D levels for most people in modern indoor-dominant lifestyles. Vitamin D3 (cholecalciferol) is more effective than D2 (ergocalciferol) at raising and maintaining serum 25(OH)D levels. Vitamin D3 should ideally be taken with a meal containing fat to maximize absorption. The dosage required to achieve optimal levels varies significantly by individual – based on starting level, body weight, sun exposure, and genetics. A reasonable starting dose for adults with documented deficiency is 2000-4000 IU/day; higher doses (4000-8000 IU/day) may be needed for those who are significantly deficient, obese, or have malabsorption. The only reliable way to know your dose is working is to retest 25(OH)D after 8-12 weeks of supplementation.
Vitamin K2 (MK-7 form) is increasingly recommended alongside vitamin D supplementation because vitamin D increases calcium absorption and K2 helps direct that calcium to bones rather than arterial walls. Magnesium is required for vitamin D activation and is commonly co-deficient with vitamin D. Addressing all three (D3, K2, and magnesium) together provides more comprehensive bone and cardiovascular benefit than vitamin D alone.
Frequently Asked Questions
How much vitamin D should I take?
This is one of the most common vitamin D questions – and the honest answer is that the right dose cannot be determined without measuring your blood level. Two people taking the same 2000 IU/day supplement can have very different 25(OH)D levels based on body weight, baseline status, sun exposure, and genetics. Dose-to-level response varies 3-4 fold between individuals. Test your level, supplement based on your result and target (40-70 ng/mL for most adults), and retest after 8-12 weeks to confirm you have reached your target. Then continue at that dose with annual monitoring.
Can I get enough vitamin D from food?
For most people, no. Very few foods contain significant amounts of vitamin D: fatty fish (salmon, mackerel, tuna) provide 400-700 IU per serving; egg yolks contain 40-50 IU; fortified milk and orange juice provide about 100 IU per cup. Reaching even 1000-2000 IU/day from food alone requires several servings of fatty fish daily – an unrealistic diet for most people. Dietary vitamin D is a meaningful contributor to status but is insufficient as the primary source for achieving optimal levels in most adults. The combination of strategic sun exposure (when available) and targeted supplementation guided by testing is the most reliable approach.
What are the signs of vitamin D deficiency?
Vitamin D deficiency is often asymptomatic or causes vague symptoms easily attributed to other causes: generalized fatigue, bone pain or muscle aches (often diffuse), muscle weakness, frequent illness or slow recovery from infections, low mood or depression, and impaired cognitive function. Bone pain and muscle weakness are more common with severe deficiency. The subtler symptoms of insufficiency (20-30 ng/mL range) – reduced athletic performance, longer illness duration, mood changes – are easily overlooked without testing. This is why blood testing is the only reliable way to assess vitamin D status: symptoms alone are inadequate to identify deficiency in most people.
Is vitamin D toxicity a real concern?
Vitamin D toxicity (hypervitaminosis D) is real but rare. It requires sustained very high supplementation – generally above 10,000-40,000 IU/day for months, producing 25(OH)D levels above 150 ng/mL (375 nmol/L). Toxicity manifests through hypercalcemia (high blood calcium): nausea, vomiting, weakness, confusion, and in severe cases kidney injury. Standard supplementation doses of 2000-8000 IU/day rarely produce 25(OH)D above 80-100 ng/mL in adults even with long-term use. Monitoring blood levels annually with doses above 4000 IU/day is prudent, but vitamin D toxicity from moderate supplementation guided by blood testing is extremely uncommon.
Does vitamin D affect testosterone and hormone levels?
Evidence suggests vitamin D has a positive relationship with testosterone levels in men. Vitamin D receptors are present in the Leydig cells of the testes (which produce testosterone), and observational studies consistently show higher vitamin D levels correlating with higher testosterone. A randomized controlled trial found that daily vitamin D3 supplementation (3332 IU/day) significantly increased total testosterone, free testosterone, and bioactive testosterone in men with vitamin D insufficiency. Whether this relationship is causal or partially confounded by factors like physical activity and overall health behaviors remains an active area of research, but the mechanistic plausibility and observational consistency make it a reasonable additional rationale for vitamin D optimization in men.
Testing Vitamin D With ApexBlood
ApexBlood’s comprehensive panel includes serum 25-hydroxyvitamin D – the correct form to measure for vitamin D status assessment. We measure the clinically relevant 25(OH)D form (not 1,25-dihydroxyvitamin D, which is active hormone but a poor indicator of body stores and is only appropriate for specific clinical scenarios). Our physicians provide personalized interpretation against the optimal range (40-70 ng/mL for most adults) rather than simply the reference range, alongside recommendations for supplementation dose and retest timing specific to your level and goals.
Get comprehensive testing for $189
The Bottom Line on Vitamin D
Vitamin D is not just a bone health nutrient – it is a master regulatory hormone precursor with functions in immune defense, muscle performance, metabolic health, mood, cognitive function, and longevity. The conventional threshold of 20 ng/mL is designed to prevent bone disease, not to optimize the full spectrum of vitamin D’s biological functions. The optimal range for comprehensive health benefits – 40-70 ng/mL – is where most health-conscious individuals should aim to be, and most are not there without supplementation. Testing is the only way to know your status. Supplementing without testing is guessing. Testing, optimizing, and retesting is how you ensure this foundational nutrient is working in your favor. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Vitamin D supplementation and blood level targets should be discussed with qualified healthcare providers. Never self-treat suspected deficiency based solely on symptoms. Always consult licensed medical professionals for diagnosis and treatment guidance.