
MCV – mean corpuscular volume – is the average size of your red blood cells, and it is one of the most informative indices on a complete blood count for diagnosing the underlying cause of anemia. While hemoglobin tells you whether you are anemic, MCV tells you why. Small red blood cells (microcytic anemia, low MCV) have a very different set of causes than large red blood cells (macrocytic anemia, high MCV) – and the distinction drives completely different diagnostic and treatment pathways. For anyone serious about energy, performance, and recovery, understanding what MCV reveals about red blood cell health and nutrient status is foundational to optimizing oxygen delivery to working tissues.
What Is MCV?
Mean corpuscular volume measures the average volume of individual red blood cells in femtoliters (fL) – one femtoliter being one quadrillionth of a liter. Red blood cells are biconcave discs approximately 6-8 micrometers in diameter optimized for carrying and releasing oxygen. Their size is precisely regulated – too small and they cannot carry sufficient hemoglobin; too large and they cannot deform properly to squeeze through capillaries and release oxygen to tissues.
MCV is automatically calculated by modern hematology analyzers from a large sample of red blood cells – typically measuring hundreds of thousands of cells and reporting the arithmetic mean. MCV is interpreted alongside MCH (mean corpuscular hemoglobin – the average hemoglobin content per red blood cell) and MCHC (mean corpuscular hemoglobin concentration – hemoglobin relative to cell volume) to characterize anemia and guide diagnosis. Together these indices are called the red blood cell indices and they transform a simple hemoglobin measurement into a diagnostic classification.
Why MCV Matters for Performance and Energy
Red blood cell optimization is central to athletic performance and daily energy levels. Hemoglobin within red blood cells is the molecule that binds oxygen in the lungs and delivers it to tissues – including working muscles during exercise. Optimal red blood cell size, shape, and hemoglobin content ensures maximum oxygen-carrying capacity and efficient oxygen release. When MCV is abnormal – too small or too large – it almost always reflects an underlying nutritional deficiency or disease process that is impairing optimal red blood cell production.
For endurance athletes and performance-focused individuals, MCV abnormalities can manifest as reduced VO2 max, faster fatigue, slower recovery, brain fog, and impaired endurance before anemia becomes severe enough to show on hemoglobin alone. Catching and correcting iron deficiency (causing microcytic cells) or B12/folate deficiency (causing macrocytic cells) early – before hemoglobin falls significantly – preserves peak performance and prevents the gradual decline that many attribute to overtraining or aging.
Normal vs. Optimal MCV Levels
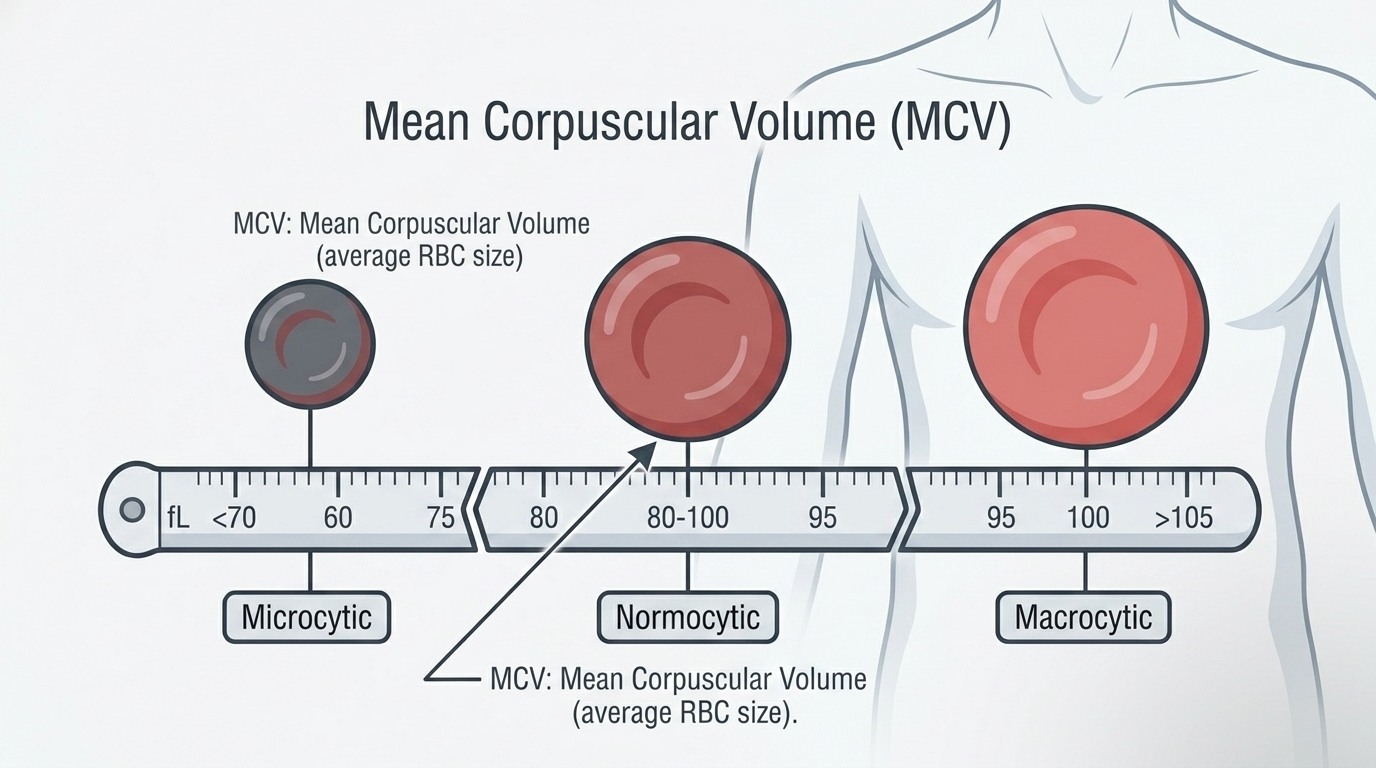
Standard Reference Ranges: Most laboratories report MCV as normal between 80 and 100 fL, with some labs extending the upper limit to 96-98 fL. These ranges capture the central 95% of the healthy adult population. MCV below 80 fL is microcytic (abnormally small cells). MCV above 100 fL is macrocytic (abnormally large cells). MCV in the 80-100 fL range is normocytic (normal-sized cells).
The Problem With “Normal”: An MCV within the reference range does not guarantee optimal red blood cell production. Iron deficiency causes MCV to fall progressively – but MCV may remain technically normal (just trending lower over months) while iron stores are substantially depleted and performance is already compromised. Similarly, combined nutritional deficiencies (such as simultaneous iron deficiency and B12 deficiency) can balance each other out, producing a normal-appearing MCV while red blood cell production is meaningfully impaired. The trend of MCV over serial measurements and its relationship to iron studies and B12/folate levels is more informative than any single MCV value.
Optimal MCV for Performance: For most adults, an MCV of 85-95 fL alongside normal hemoglobin, ferritin, B12, and folate suggests healthy red blood cell production. MCV trending toward either end of the normal range (below 85 or above 95) warrants checking the complementary iron and B12 biomarkers before the trend progresses to frank anemia.
What Causes Low MCV (Microcytic Anemia)?
Iron deficiency is the most common cause of low MCV worldwide and the most common nutritional deficiency in endurance athletes. Iron is required for hemoglobin synthesis – without adequate iron, the bone marrow produces smaller red blood cells with less hemoglobin. Iron deficiency progresses in stages: depleted iron stores (low ferritin) occur first, followed by iron-deficient erythropoiesis (low iron/high TIBC, falling MCV), and finally iron-deficiency anemia (low hemoglobin, clearly microcytic cells). MCV falls relatively late in the progression, meaning iron stores can be substantially depleted with MCV still near-normal.
Thalassemia – particularly alpha and beta thalassemia trait – is a genetic condition causing microcytosis that is common in people of Mediterranean, Middle Eastern, Southeast Asian, and African ancestry. Unlike iron deficiency, ferritin is normal or elevated in thalassemia and supplemental iron does not help. Distinguishing thalassemia trait from iron deficiency requires checking ferritin and iron studies. Anemia of chronic disease (from inflammation, infection, cancer, autoimmune disease) can cause microcytosis but more commonly produces normocytic anemia. Sideroblastic anemia from lead poisoning, alcohol, or certain medications is a rarer cause.
What Causes High MCV (Macrocytic Anemia)?
Vitamin B12 deficiency is a leading cause of macrocytosis and can develop insidiously over years as body stores deplete. B12 is required for DNA synthesis – without adequate B12, cells cannot divide normally and instead grow large without dividing, producing oversized red blood cells. B12 deficiency is particularly common in vegans and vegetarians (B12 is found almost exclusively in animal products), people over 65 (reduced gastric acid and intrinsic factor decrease absorption), people on metformin (which impairs B12 absorption), and anyone with digestive conditions impairing absorption (Crohn’s disease, celiac, previous gastric surgery). B12 deficiency can also cause progressive neurological damage that may be irreversible if untreated.
Folate (vitamin B9) deficiency similarly impairs DNA synthesis and causes macrocytosis. Folate deficiency is common in people with poor vegetable intake, alcohol use disorder (alcohol impairs folate absorption and metabolism), pregnancy (dramatically increased folate demand), malabsorption syndromes, and use of certain medications (methotrexate, trimethoprim, phenytoin). Alcohol is a major cause of macrocytosis independent of folate – alcohol directly impairs red blood cell maturation. Hypothyroidism slows cell production and increases MCV. Liver disease impairs red blood cell membrane formation. Certain medications (hydroxyurea, azathioprine, chemotherapy drugs) directly impair DNA synthesis and cause macrocytosis.
Frequently Asked Questions
Can I have iron deficiency with a normal MCV?
Yes, and this is common. MCV is one of the last CBC markers to change in iron deficiency – ferritin (iron stores) falls first, followed by serum iron and TIBC changes, and finally hemoglobin and MCV decline. Many athletes and women of reproductive age have significantly depleted ferritin with performance impacts while their MCV remains in the 80-90 fL range. This is why ferritin is the most sensitive early marker of iron deficiency – not MCV or hemoglobin.
How quickly does MCV normalize after treating iron or B12 deficiency?
Red blood cells survive approximately 90-120 days in circulation, so MCV normalization after correcting a deficiency takes weeks to months. After starting iron supplementation for iron deficiency, reticulocytes (young red blood cells) begin increasing within 5-7 days, and hemoglobin typically starts rising within 2-4 weeks, but MCV may take 2-3 months to fully normalize as the population of new, properly sized cells gradually replaces the old microcytic cells. B12 treatment similarly shows progressive improvement over months.
What is the difference between MCV and MCH?
MCV measures cell size (volume in fL). MCH (mean corpuscular hemoglobin) measures the average amount of hemoglobin per individual red blood cell in picograms (pg). Because hemoglobin occupies a fixed percentage of the cell interior, MCV and MCH typically move together – microcytic cells tend to be hypochromic (low MCH) and macrocytic cells tend to have higher MCH. They provide complementary information. MCHC (mean corpuscular hemoglobin concentration) measures hemoglobin relative to cell volume as a percentage – it is the most sensitive indicator of hemoglobin packing density and the most specific indicator of true iron deficiency when low.
Should vegans and vegetarians check MCV regularly?
Yes. People on plant-based diets are at elevated risk for both B12 deficiency (no dietary B12 in plants) and iron deficiency (plant-based iron is non-heme iron with significantly lower bioavailability than heme iron from meat). MCV is a downstream indicator of these deficiencies – B12 and folate (for macrocytosis) and ferritin/iron studies (for microcytosis) should be checked alongside MCV. Annual or biannual monitoring with a comprehensive panel allows early correction before deficiencies become clinically significant.
Testing MCV With ApexBlood
MCV is included in ApexBlood’s comprehensive CBC panel alongside MCH, MCHC, hemoglobin, ferritin, and full iron studies – giving you the complete picture needed to diagnose the cause of any abnormal MCV rather than just flagging that one exists. Our physicians can interpret your red blood cell indices in the context of your diet, training load, and complete metabolic profile to identify what is driving any abnormality and guide targeted correction.
Get comprehensive testing for $189
The Bottom Line on MCV
MCV is a powerful diagnostic tool that transforms a simple red blood cell count into a classified anemia type with a defined set of causes. Low MCV points toward iron deficiency, thalassemia, or chronic disease. High MCV points toward B12 deficiency, folate deficiency, alcohol, hypothyroidism, or liver disease. Normal MCV does not rule out nutritional deficiencies – ferritin and B12 levels provide earlier detection. For anyone serious about energy, performance, and cognitive function, optimizing the entire red blood cell system – not just flagging when hemoglobin drops below normal – is what separates peak function from gradual decline. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. MCV and red blood cell indices require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.