
Iron saturation – also called transferrin saturation – is the percentage of your iron-carrying protein that is actually loaded with iron right now. It is one of the most direct, real-time windows into your iron delivery system available from a standard blood panel. Low iron saturation tells you that iron is not reaching your tissues efficiently. High iron saturation tells you that iron is saturating the transport system – and potentially spilling into places it does not belong. Neither extreme is optimal, and the “normal” range on your lab report gives you almost no guidance about where you actually want to be for performance and longevity.
What Is Iron Saturation?
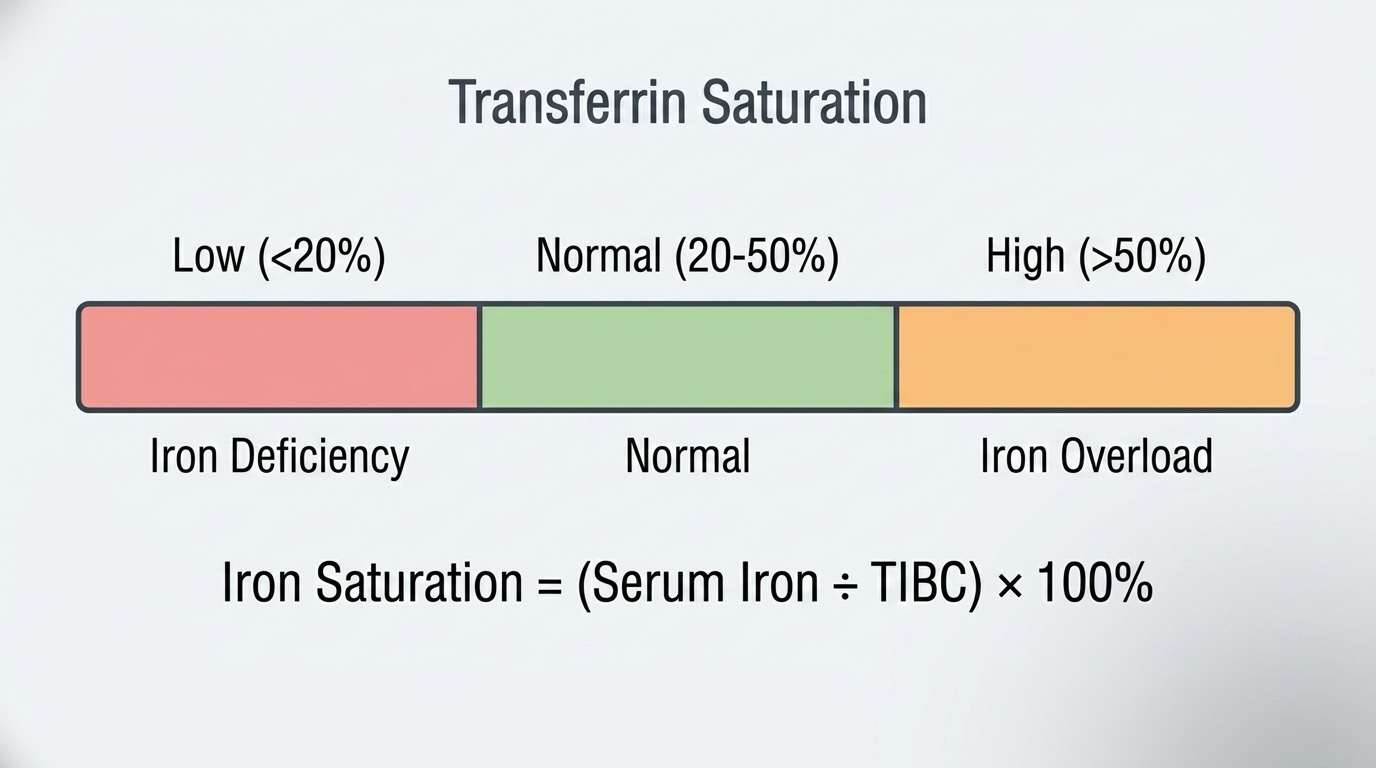
Iron saturation (transferrin saturation) is the ratio of serum iron to TIBC (Total Iron Binding Capacity), expressed as a percentage. The formula is: Iron Saturation (%) = (Serum Iron / TIBC) x 100. Transferrin is the protein that transports iron through your bloodstream. Each transferrin molecule can bind two iron atoms. Iron saturation tells you what fraction of transferrin’s total binding capacity is currently occupied by iron – essentially, how full your iron delivery trucks are.
If iron saturation is 20%, it means 20% of transferrin’s binding capacity is carrying iron and 80% is empty – traveling through your blood waiting for iron that is not available. If iron saturation is 60%, transferrin is heavily loaded with iron, which in certain contexts indicates that iron is being absorbed faster than it can be safely stored and may be accumulating in organs. Iron saturation is not a static number – it varies throughout the day, typically being highest in the morning after an overnight fast, which is why iron panels should ideally be drawn fasting in the morning for consistent, comparable results.
Why Iron Saturation Matters for Performance
Iron saturation matters because it reflects real-time iron delivery efficiency. You can have ferritin at a reasonable level while iron saturation is low – meaning iron is stored but is not being released into circulation effectively. This functional iron deficiency can occur with chronic inflammation, which traps iron inside storage proteins to deny it to pathogens during infection. The inflammatory response is biologically intelligent but sometimes creates a situation where iron stores look adequate while tissue iron delivery is genuinely impaired.
For athletes and high performers, iron saturation in the optimal range ensures that iron is flowing efficiently to bone marrow for red blood cell production, to muscle mitochondria for energy metabolism, and to the enzymes throughout your body that require iron as a cofactor. Low iron saturation – whether from iron deficiency or inflammation-driven functional deficiency – impairs all of these processes and shows up as fatigue, poor exercise tolerance, slow recovery, and cognitive dulling long before anemia develops.
Normal vs. Optimal Iron Saturation
Standard Reference Ranges: Most laboratories report iron saturation as normal between 20% and 50% for men and 15% and 50% for women. These ranges are designed to flag clear abnormalities rather than guide optimization. Transferrin saturation below 20% is the threshold at which iron deficiency begins to impair red blood cell production. Above 50% raises concern for iron overload. But between 20% and 50%, the range is wide enough to encompass both well-optimized and suboptimal iron delivery.
The Problem With “Normal”: Iron saturation at 22% and iron saturation at 45% are both “normal” by standard lab criteria. They describe radically different physiological situations. At 22%, a meaningful fraction of your iron transport capacity is working at very low efficiency – your body is reaching for iron that barely meets current needs. At 38%, your iron delivery system is running efficiently with adequate iron available for all tissues. The number within the “normal” range matters enormously for how you actually feel and perform.
Optimal Iron Saturation for Performance: For most healthy adults, iron saturation between 25% and 40% reflects efficient iron delivery alongside adequate stores. Below 20% – especially combined with low ferritin – confirms iron deficiency that warrants intervention. Above 45-50% – especially with elevated ferritin – raises concern for iron overload and warrants investigation for hemochromatosis or other iron accumulation disorders. The optimal zone gives your tissues reliable iron access without the oxidative damage risk of iron excess.
What Causes Low Iron Saturation?
Iron deficiency is the most common cause – when iron stores are depleted, less iron is available to bind transferrin, and saturation falls. Iron deficiency from inadequate dietary intake, blood loss (heavy menstruation, GI bleeding), poor absorption (celiac disease, inflammatory bowel disease), or the high iron demands of endurance athletics are the most common drivers. Chronic inflammation also drives low iron saturation through a different mechanism: the body actively withholds iron from circulation during inflammatory states, reducing transferrin saturation even when ferritin may appear normal or elevated. This is why iron saturation is a more sensitive functional indicator than ferritin alone in people with underlying inflammatory conditions. Hypothyroidism can also lower iron saturation by reducing iron absorption efficiency in the gut.
What Causes High Iron Saturation?
Hereditary hemochromatosis is the most important cause of persistently elevated iron saturation to identify – this genetic condition causes progressive iron accumulation in organs and is treatable with regular therapeutic phlebotomy when caught early. Iron saturation above 45% consistently, especially combined with elevated ferritin, should prompt genetic testing for the HFE gene mutations associated with hemochromatosis. Other causes of elevated iron saturation include iron supplementation beyond what the body needs, liver disease (which impairs iron storage and allows iron to accumulate in circulation), acute hepatitis (which releases stored iron into the bloodstream), and certain hemolytic anemias where red blood cell destruction releases iron. Iron saturation is naturally higher in the morning and fluctuates throughout the day, so a single mildly elevated value requires repeat testing before conclusions are drawn.
Iron Saturation and the Full Iron Panel
Iron saturation reaches its full interpretive power when read alongside ferritin, serum iron, and TIBC. The classic iron deficiency pattern shows low iron saturation (below 20%), low ferritin, low serum iron, and high TIBC. The classic iron overload pattern shows high iron saturation (above 45-50%), high ferritin, high serum iron, and low TIBC. Anemia of chronic disease shows low iron saturation and low serum iron despite normal or elevated ferritin and normal or low TIBC – because inflammation is functionally withholding iron from circulation while keeping it stored. Each pattern points toward a completely different clinical response, and getting this distinction right prevents the common error of supplementing iron when inflammation – not depletion – is the real problem.
Frequently Asked Questions
What iron saturation level is optimal for performance?
For most adults focused on performance, iron saturation between 25% and 40% reflects efficient iron delivery without the risks of iron excess. Below 20% indicates iron deficiency affecting iron delivery regardless of what ferritin shows. Above 45-50% warrants investigation for iron overload. The optimal zone is where your transport system is adequately loaded and running efficiently – enough iron to fill tissues’ needs without saturating the system to the point where iron spills into unprotected spaces.
Can iron saturation be low even if ferritin is normal?
Yes, and this is clinically important. Chronic inflammation can produce low iron saturation with normal or elevated ferritin because the inflammatory response actively withholds iron from circulation while keeping it locked in storage proteins. This is called functional iron deficiency or anemia of chronic disease. People in this pattern are often told their iron is “fine” because their ferritin is normal, but their tissues may be functionally iron-deprived because iron saturation is suppressed by inflammation.
Should I take iron supplements if my iron saturation is low?
Not necessarily, and not without understanding why it is low first. If iron saturation is low due to true iron deficiency (also reflected in low ferritin), iron supplementation is appropriate. If iron saturation is low due to inflammation driving functional deficiency, supplementing iron without addressing the inflammation is likely to be ineffective and may contribute to oxidative damage. Always confirm the pattern with a full iron panel before supplementing, and work with a physician to identify the underlying cause.
Does iron saturation vary throughout the day?
Yes, significantly. Iron saturation is highest in the morning and can be 30-40% lower in the afternoon and evening. This diurnal variation means that iron panels drawn at different times of day are not directly comparable. For consistent, reproducible results, iron panels should be drawn fasting in the morning – ideally before 10am. A single afternoon value showing borderline elevation should be repeated with a morning fasting draw before conclusions are drawn.
What iron saturation level suggests hemochromatosis?
Transferrin saturation consistently above 45% on a fasting morning draw – especially combined with elevated ferritin – is the primary screening signal for hereditary hemochromatosis. A single elevation does not confirm the diagnosis, but repeated fasting iron saturations above 45% should prompt HFE gene mutation testing. Hemochromatosis is one of the most common genetic disorders in people of Northern European descent, affects roughly 1 in 200 people, and is highly treatable when identified early through therapeutic phlebotomy.
Testing Iron Saturation With ApexBlood
Iron saturation is reported as part of ApexBlood’s complete iron status panel, calculated from your serum iron and TIBC alongside ferritin and UIBC. The complete iron panel gives each individual marker the context it needs to be properly interpreted – a single iron saturation number without the full panel is like reading one sentence from a paragraph and guessing at the plot. Our physicians interpret the complete picture and can discuss targeted interventions based on what your specific pattern indicates.
You cannot optimize what you do not measure. Understand where your iron delivery system actually stands before guessing at interventions.
Get comprehensive testing for $189
The Bottom Line on Iron Saturation
Iron saturation is a real-time snapshot of how efficiently iron is moving through your bloodstream to the tissues that need it. The “normal” range of 20-50% is too broad to guide optimization – both extremes of “normal” represent meaningfully different physiological states with different performance implications. Optimal iron saturation (25-40%) means your iron delivery system is running efficiently. Outside that range, understanding the why matters more than chasing a number.
Test comprehensively, interpret your full iron panel in context, and work with physicians who understand the difference between normal and optimal. Stop accepting “your iron is fine” when optimal delivery could unlock performance you have been leaving on the table. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Iron saturation and iron status require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.