
ALT – alanine aminotransferase – is the most liver-specific enzyme on a standard metabolic panel, and it is often the first biomarker to signal that something is damaging your liver cells. If there is one liver enzyme to pay close attention to, it is ALT. Unlike AST (which also comes from skeletal muscle and heart), ALT is found primarily in the liver, making elevated ALT a much more specific indicator of hepatocellular injury. But here is what conventional medicine often gets wrong about ALT: the standard “normal” reference ranges are based on population averages that include people with subclinical fatty liver disease – which means “normal” ALT by lab standards may include levels at which significant liver inflammation and early fibrosis are already occurring. For anyone serious about metabolic health and longevity, optimal ALT is not just “below the upper limit of normal.”
What Is ALT?
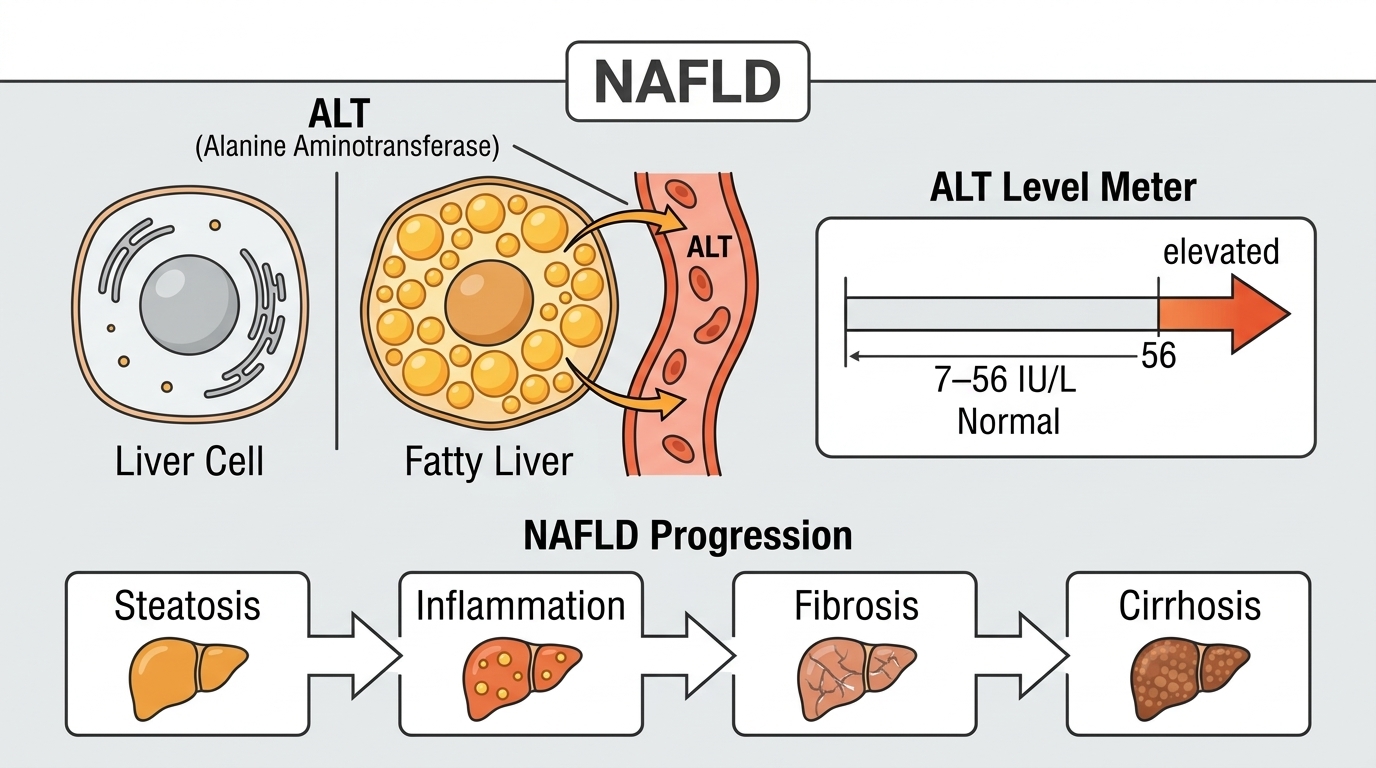
Alanine aminotransferase (ALT, previously known as SGPT – serum glutamic-pyruvic transaminase) is an enzyme that plays a role in gluconeogenesis – the liver’s process of making glucose from amino acids. It facilitates the transfer of an amino group from alanine to alpha-ketoglutarate, producing pyruvate that can enter glucose synthesis. ALT is concentrated in the cytoplasm of liver cells (hepatocytes), with substantially lower concentrations in the kidneys, heart, skeletal muscle, and other organs. This relative hepatic specificity makes ALT the preferred single enzyme marker for evaluating liver health.
When liver cells are damaged or destroyed – by fat accumulation, alcohol toxicity, viral infection, drug toxicity, or autoimmune attack – the cell membrane becomes permeable and ALT leaks into the bloodstream. The degree of elevation generally correlates with the amount of ongoing liver cell damage: mild elevations suggest ongoing inflammation with early cell damage, very high elevations (above 1,000 U/L) suggest acute massive liver injury. ALT has a serum half-life of approximately 47 hours, longer than AST, meaning it remains elevated longer after an acute injury and is more useful for detecting subacute or chronic liver damage.
Why ALT Matters for Performance and Longevity
Non-alcoholic fatty liver disease (NAFLD) is the most common liver disease in the world, affecting 25-30% of adults in Western populations and up to 70-80% of people with obesity and type 2 diabetes. ALT is the primary blood biomarker for NAFLD – it is often the first and sometimes the only routine test that signals developing liver disease. Elevated ALT from NAFLD precedes cirrhosis and liver failure by years to decades, which is why identifying and reversing it early – when the liver can still regenerate fully – is so clinically important.
For high performers, ALT matters beyond just “avoiding liver disease.” The liver is central to metabolism, hormone clearance, drug metabolism, energy production, and detoxification. A liver under inflammatory stress – even subclinically, reflected by persistently elevated ALT – is a metabolically compromised liver that does not perform these functions at peak efficiency. Optimizing liver health through dietary choices, alcohol moderation, metabolic weight management, and avoiding hepatotoxic medications and supplements is one of the most high-leverage metabolic health interventions available.
Normal vs. Optimal ALT Levels
Standard Reference Ranges: Most laboratories report ALT as normal up to 40-56 U/L for men and 31-45 U/L for women, with some variation between labs. These ranges were established from population samples that include people with subclinical NAFLD – a significant methodological problem that has been widely recognized in the hepatology literature. Because a substantial fraction of the “healthy” population used to establish reference ranges has early-stage fatty liver disease, the upper limit of “normal” is higher than it would be if only truly metabolically healthy people were included.
The Problem With “Normal”: Multiple liver disease specialists and research groups have argued that the standard ALT upper limits of normal are too high – that significant liver inflammation and early fibrosis can occur with ALT values well within the reference range. A 2002 study found that the truly normal ALT (in people with no liver risk factors and no metabolic disease) should be closer to 30 U/L for men and 19 U/L for women. Using these more stringent criteria would identify three to four times as many people with liver disease as the current upper limits of normal.
Optimal ALT for Metabolic Health: For most metabolically healthy adults, ALT below 25-30 U/L for men and below 20 U/L for women suggests healthy hepatocellular integrity without significant ongoing liver inflammation. ALT consistently above 30-35 U/L – even within the laboratory reference range – warrants metabolic investigation including assessment of insulin resistance, visceral adiposity, alcohol intake, and medication or supplement effects. The trend over time matters enormously: a rising ALT from 20 to 35 U/L over two years is a signal to act, not to wait until it crosses the “normal” threshold.
What Causes Elevated ALT?
Non-alcoholic fatty liver disease (NAFLD) is by far the most common cause of mildly to moderately elevated ALT in the outpatient setting – driven by visceral adiposity, insulin resistance, high sugar and refined carbohydrate intake, and metabolic syndrome. Alcoholic liver disease causes ALT elevation with a characteristic pattern (AST/ALT ratio above 2:1 in alcoholic hepatitis). Viral hepatitis – particularly hepatitis C, which can smolder for decades before causing obvious symptoms – is an important and often unrecognized cause of chronically elevated ALT. Autoimmune hepatitis (particularly common in women) causes ALT elevation with positive autoantibodies. Drug-induced liver injury from medications (acetaminophen at high doses, statins, antibiotics, antifungals, anti-seizure medications) and supplements (herbal and dietary supplements cause roughly 20% of acute liver failure cases in the US) is a common and underappreciated cause. Celiac disease can cause mildly elevated ALT that normalizes on a gluten-free diet. Thyroid disease (hypothyroidism) can mildly elevate ALT. Vigorous exercise elevates AST much more than ALT from skeletal muscle – if AST is elevated and ALT is proportionally much lower, exercise is the more likely driver.
How to Lower ALT and Optimize Liver Health
For NAFLD-driven ALT elevation – the most common scenario – the interventions with the strongest evidence are weight loss (even modest 5-10% body weight reduction significantly reduces liver fat and ALT in NAFLD), dietary sugar and refined carbohydrate reduction (fructose in particular drives de novo lipogenesis in the liver), alcohol elimination or significant reduction, coffee consumption (genuinely hepatoprotective – multiple studies show 2-4 cups daily reduces liver fibrosis risk), regular aerobic exercise (reduces liver fat independent of weight loss), and treating underlying insulin resistance. Medications approved for NAFLD are emerging but lifestyle modification remains the most effective intervention. GLP-1 weight loss medications have shown remarkable efficacy for liver fat reduction and ALT normalization as a secondary benefit of their metabolic effects. Metformin may modestly benefit liver health in insulin-resistant individuals. Identifying and stopping any hepatotoxic medications or supplements is essential when drug-induced liver injury is suspected.
Frequently Asked Questions
What ALT level should I aim for?
Many hepatologists recommend targeting ALT below 25-30 U/L for men and below 19-20 U/L for women as indicators of optimal liver health – values lower than most lab reference ranges suggest. The standard “normal” cutoffs (up to 40-56 U/L) were established from populations that include people with subclinical fatty liver disease, making them a poor guide for optimization. If your ALT is between 20 and 45 U/L, it may be within “normal” but is worth investigating for metabolic drivers.
Can ALT be elevated without symptoms?
Yes – this is exactly what makes it valuable. NAFLD, chronic hepatitis C, early alcoholic liver disease, and drug-induced liver injury often produce elevated ALT without any symptoms. The liver has no pain receptors, and liver disease is notoriously asymptomatic until it reaches advanced stages like cirrhosis. Routine ALT monitoring catches liver injury early – when it is most reversible – rather than waiting for symptoms to develop.
Can I lower my ALT through diet alone?
For NAFLD-driven ALT elevation, dietary changes are highly effective. The most impactful interventions are reducing added sugar and fructose (cutting out soda, fruit juice, and processed sweets), reducing refined carbohydrates, adopting a Mediterranean-style or low-carbohydrate eating pattern, eliminating or significantly reducing alcohol, and achieving modest weight loss if overweight. Studies show ALT can normalize within 3-6 months of aggressive lifestyle modification in early NAFLD.
Does alcohol affect ALT?
Yes, significantly. Even moderate alcohol consumption elevates ALT in some individuals. Heavy drinking causes alcoholic liver disease with the characteristic pattern of AST higher than ALT (AST/ALT ratio above 2:1). Abstaining from alcohol for 4-6 weeks before a liver function panel gives the cleanest baseline for assessing non-alcohol-related liver health. If ALT is elevated and you drink regularly, alcohol reduction is always the first intervention to try before investigating other causes.
Do statins elevate ALT?
Statins can mildly elevate ALT in some people – occurring in roughly 1-3% of statin users. The elevation is usually mild (less than 3x the upper limit of normal) and often transient. Significant statin-induced liver injury is rare but real, typically occurring within the first year of use. For people on statins with mildly elevated ALT, baseline liver function testing before starting and at 3-6 months after initiating therapy is appropriate monitoring. Routine ongoing liver testing for stable statin users with normal initial values is no longer recommended by most guidelines.
Testing ALT With ApexBlood
ALT is a core component of ApexBlood’s comprehensive panel alongside AST, ALP, bilirubin, albumin, and metabolic markers including glucose, insulin, and lipids that provide the full metabolic context for interpreting liver health. Because NAFLD is the most common cause of elevated ALT and is driven by metabolic dysfunction, seeing ALT alongside your insulin resistance markers, lipids, and inflammatory indicators tells the complete story. Our physicians can discuss what your ALT trend means for your metabolic and liver health and recommend targeted interventions based on your complete picture.
You cannot optimize what you do not measure. For metabolic health and longevity, understanding your true liver health status – not just whether you clear the population-based “normal” threshold – is essential.
Get comprehensive testing for $189
The Bottom Line on ALT
ALT is the most liver-specific enzyme on your panel and one of the most actionable biomarkers for metabolic health optimization. The “normal” reference range is genuinely too permissive – established from populations that include people with early fatty liver disease. Optimal ALT is in the lower portion of the reference range: below 25-30 U/L for men and below 19-20 U/L for women. A rising ALT trend is a call to action – to address insulin resistance, reduce dietary sugar, moderate alcohol, review medications and supplements, and optimize body composition before subclinical liver inflammation progresses to significant fibrosis. Stop accepting “your liver enzymes are in the normal range” when your ALT is trending upward. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. ALT and liver health require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.