
Blood Urea Nitrogen – BUN – is a kidney function marker that is included on virtually every standard blood panel, yet most people have little understanding of what it actually measures or what drives it. BUN reflects the amount of urea nitrogen circulating in your blood – a byproduct of protein metabolism that the kidneys continuously filter and excrete. Elevated BUN can mean your kidneys are not clearing waste efficiently. But BUN can also be elevated from dehydration, high protein intake, gastrointestinal bleeding, or physical and metabolic stress – with perfectly normal kidney function. Low BUN can indicate malnutrition, liver disease, or overhydration. BUN in isolation is a limited test. BUN in context with creatinine, eGFR, and your clinical picture becomes genuinely informative for assessing kidney health and protein metabolism.
What Is BUN?
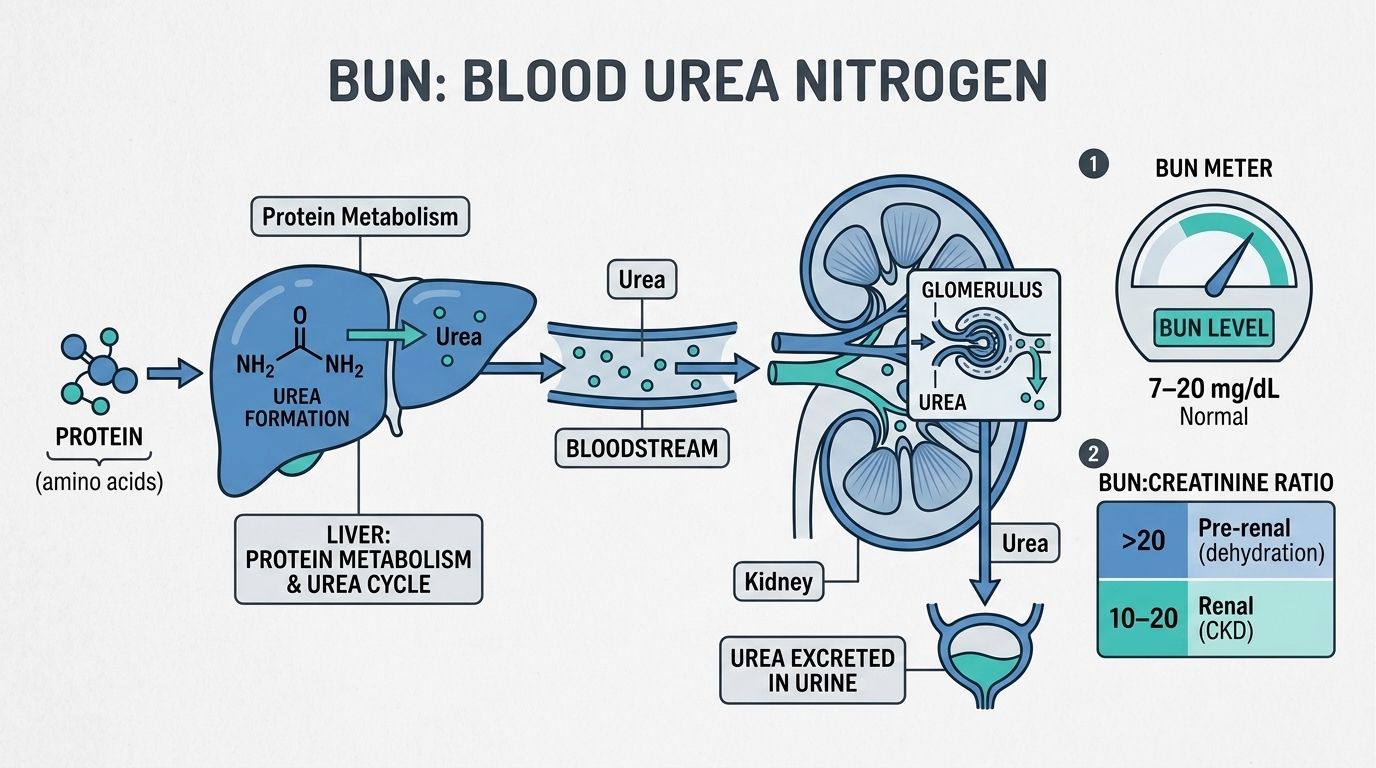
Urea is the primary end-product of protein catabolism in your body. When protein is broken down – from dietary intake, muscle turnover, or tissue breakdown – the amino acids are metabolized, releasing nitrogen. The liver converts this nitrogen to urea through the urea cycle, releasing it into the bloodstream. The kidneys continuously filter blood urea and excrete it in urine. BUN (blood urea nitrogen) measures the concentration of the nitrogen portion of urea in your bloodstream – a proxy for how much urea is circulating and how efficiently the kidneys are removing it.
Because BUN reflects both production (how much protein is being catabolized) and excretion (how well the kidneys are clearing urea), it is influenced by multiple factors beyond kidney function alone. High protein intake increases urea production. Dehydration decreases urine flow and increases BUN concentration. Gastrointestinal bleeding delivers large amounts of protein (from blood) to the gut for digestion, dramatically increasing urea production. Reduced kidney function decreases urea excretion, allowing it to accumulate. Understanding which factor is driving any BUN abnormality requires the BUN/creatinine ratio and clinical context.
Why BUN Matters for Performance and Kidney Health
For high performers and health optimizers, BUN provides two distinct types of insight. First, it is a kidney function screening marker – rising BUN alongside rising creatinine and falling eGFR signals declining kidney filtration capacity that warrants investigation and intervention before significant permanent damage occurs. Chronic kidney disease affects roughly 15% of US adults and is substantially underdiagnosed because it is asymptomatic in its early stages. Serial BUN and creatinine monitoring is one of the ways to catch deteriorating kidney function before it becomes advanced.
Second, BUN reflects protein metabolism and nutritional state. Athletes on high-protein diets typically have higher BUN than sedentary individuals eating standard protein – not from kidney disease but from the higher protein load being metabolized. Very low BUN alongside low protein intake suggests inadequate dietary protein or reduced liver function (since the liver produces urea). For people pursuing aggressive body composition optimization or athletic performance, understanding BUN in the context of protein intake, hydration, and training intensity provides insight into protein metabolism efficiency.
Normal vs. Optimal BUN Levels
Standard Reference Ranges: Most laboratories report BUN as normal between 7 and 25 mg/dL (or 2.5-8.9 mmol/L as urea in some countries). These ranges accommodate the substantial variation in BUN from dietary protein intake and hydration status. The upper end of normal identifies significantly impaired urea clearance, while the lower end identifies markedly reduced urea production from malnutrition or liver disease.
The Importance of BUN/Creatinine Ratio: The BUN/creatinine ratio is more diagnostically useful than BUN alone. A normal ratio is approximately 10:1 to 20:1. High BUN with a high BUN/creatinine ratio (above 20:1) suggests a pre-renal cause – dehydration, high protein intake, GI bleeding, or other states increasing urea production relative to creatinine. High BUN with a normal BUN/creatinine ratio (10:1 to 20:1) suggests intrinsic kidney disease – both markers are rising proportionally because the kidneys are not filtering either effectively. Low BUN/creatinine ratio (below 10:1) may indicate malnutrition, liver disease, or a low protein diet.
Optimal BUN for Performance: For a well-hydrated adult eating moderate-to-high protein, BUN between 10 and 20 mg/dL with a normal creatinine and eGFR suggests healthy kidney function and normal protein metabolism. BUN consistently above 20 mg/dL warrants checking hydration status, protein intake, and creatinine to determine whether it reflects diet, hydration, or kidney function. BUN below 7 mg/dL warrants checking albumin and protein intake for signs of malnutrition.
What Causes High BUN?
Dehydration is the most common cause of mildly elevated BUN in otherwise healthy people – concentrated blood contains more urea per unit volume. High dietary protein intake increases urea production and raises BUN, which is why athletes on high-protein diets often have BUN in the 20-25 mg/dL range without any kidney dysfunction. Upper gastrointestinal bleeding (from ulcers, varices, or tumors) is a classic cause of dramatically elevated BUN – the blood is digested in the gut and the amino acids are processed through the urea cycle, increasing BUN without similarly elevating creatinine (hence a high BUN/creatinine ratio). Acute and chronic kidney disease impair urea excretion. Muscle breakdown (rhabdomyolysis, severe illness, major surgery) increases protein catabolism and urea production. Corticosteroids increase protein catabolism. Congestive heart failure reduces kidney perfusion. Fever and significant physiological stress increase protein breakdown.
What Causes Low BUN?
Malnutrition and severely inadequate protein intake reduce urea production because there is less protein being metabolized. Liver disease impairs the urea cycle – severely damaged livers cannot convert ammonia to urea effectively, causing ammonia accumulation (hepatic encephalopathy) alongside low BUN. Overhydration dilutes BUN. Pregnancy (hemodilution and increased renal blood flow) lowers BUN. SIADH (syndrome of inappropriate ADH secretion) causes dilutional hyponatremia and low BUN. Some athletes with excellent kidney function and high urine output have low-normal BUN that reflects efficient clearance rather than any problem.
Frequently Asked Questions
Does high protein intake damage kidneys?
In people with healthy kidneys, high protein intake does not cause kidney damage. Higher protein increases BUN (from increased urea production) and creatinine clearance (kidneys filter more), but this is a normal adaptation, not damage. The concern about protein and kidneys applies primarily to people with pre-existing chronic kidney disease – in this population, high protein intake accelerates kidney disease progression by increasing the filtration burden on already impaired nephrons. For healthy individuals, protein intakes up to 2-3 g/kg body weight have not demonstrated kidney harm in research.
How do I know if my high BUN is from dehydration or kidney disease?
Check the BUN/creatinine ratio. If BUN is high but creatinine is normal and the BUN/creatinine ratio is above 20:1, dehydration or high protein intake is the most likely explanation. If both BUN and creatinine are elevated with a ratio in the 10:1 to 20:1 range, kidney disease is more likely. Drinking additional water for 24-48 hours and re-checking BUN is a practical first step when dehydration is suspected.
Should athletes have a higher BUN?
Yes, typically. Athletes consuming 1.5-2.5 g protein per kg body weight daily will have higher BUN than sedentary individuals on standard protein intake – often in the 18-25 mg/dL range rather than the 10-15 mg/dL more common in less active people. This reflects increased protein metabolism, not kidney dysfunction. If creatinine and eGFR are normal alongside the elevated BUN, high protein intake and/or dehydration from training are the likely explanations.
What is the best way to monitor kidney health?
A comprehensive kidney health assessment includes BUN, creatinine, eGFR, urine albumin-to-creatinine ratio (uACR), and blood pressure. eGFR (estimated glomerular filtration rate) calculated from creatinine is the primary kidney function metric. Urine albumin detects early kidney damage (microalbuminuria) before eGFR declines. BUN and creatinine together with the BUN/creatinine ratio provide additional context. Trending these markers over time is more informative than any single measurement.
Testing BUN With ApexBlood
BUN is included in ApexBlood’s comprehensive panel alongside creatinine, eGFR, electrolytes, and metabolic markers that allow complete kidney health assessment. Our panel provides the full picture – not just individual numbers but the ratios and relationships that make these markers interpretable. Our physicians can discuss what any BUN abnormality likely means in the context of your protein intake, hydration, training load, and complete metabolic profile.
Get comprehensive testing for $189
The Bottom Line on BUN
BUN is a kidney filtration and protein metabolism marker that requires context – specifically the BUN/creatinine ratio, creatinine, eGFR, hydration status, and protein intake – to be properly interpreted. High BUN from dehydration or a high-protein diet requires a different response than high BUN from kidney disease. Low BUN from malnutrition requires a different response than low BUN from efficient kidney clearance. Understanding what is actually driving your BUN is more valuable than any absolute number. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. BUN and kidney health require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.