
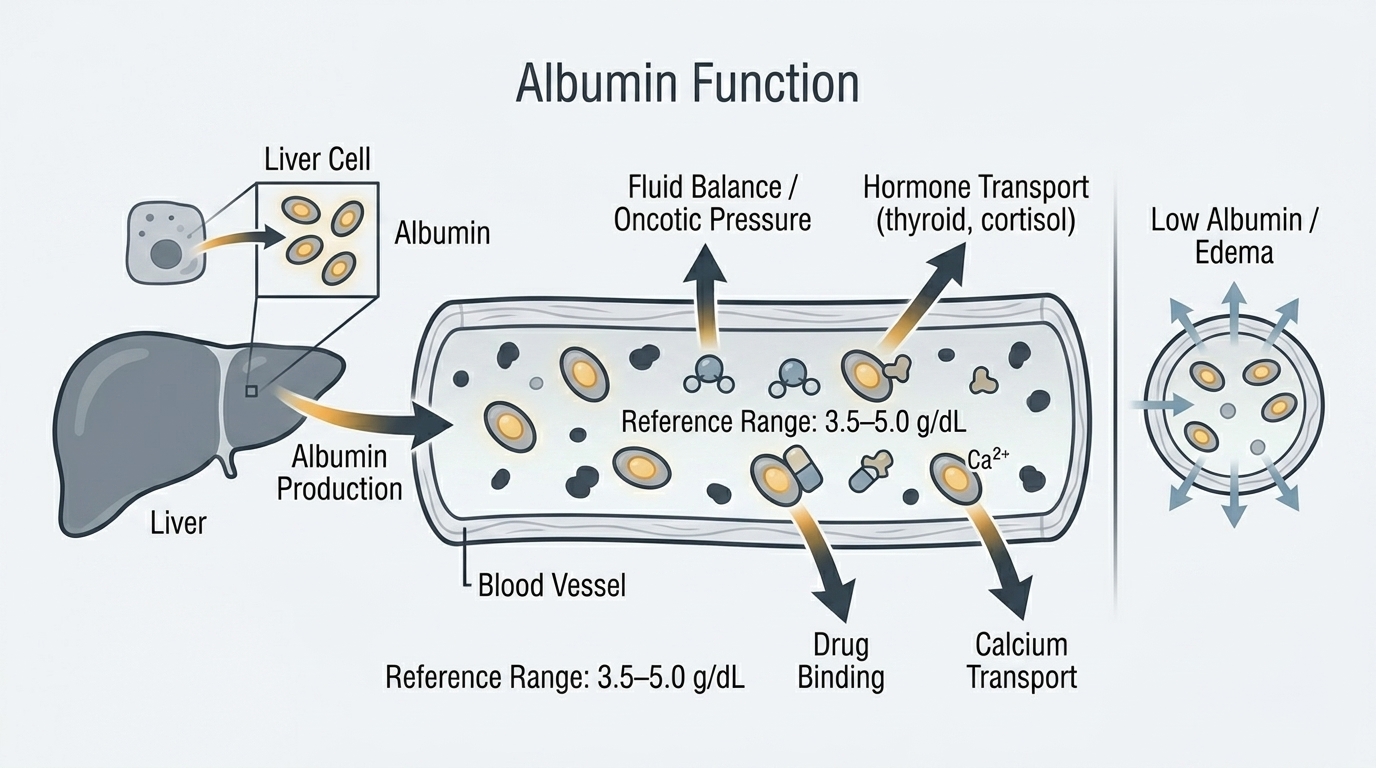
Albumin is the most abundant protein in your blood, and it is one of the most informative biomarkers on a comprehensive panel for assessing your overall health trajectory. Produced exclusively by the liver, albumin performs critical functions including maintaining the osmotic pressure that keeps fluid within blood vessels, transporting hormones, fatty acids, bilirubin, calcium, and medications through the bloodstream, and providing a reservoir of amino acids during nutritional stress. Low albumin is one of the strongest predictors of adverse outcomes across virtually every disease category studied – not because albumin itself causes harm when low, but because low albumin reflects the cumulative burden of poor nutrition, liver dysfunction, inflammation, or protein losses that undermine health and longevity. If there is one protein marker that deserves serious attention beyond a casual glance, it is albumin.
What Is Albumin?
Albumin is a soluble protein synthesized continuously by liver hepatocytes. The liver produces roughly 15 grams of albumin per day in healthy adults, with a half-life of approximately 20 days in the bloodstream. This relatively long half-life makes albumin a useful marker of nutritional and hepatic status over a 2-4 week timeframe – unlike pre-albumin (transthyretin), which has a much shorter half-life and reflects more acute changes. Because albumin takes weeks to change, a single low albumin value suggests a prolonged period of impaired synthesis or excessive losses rather than an acute event.
Approximately 60% of your total serum protein is albumin, with globulins making up the remaining 40%. Albumin is also the primary carrier protein for many important molecules: thyroid hormones, cortisol, testosterone, calcium, fatty acids, bilirubin, drugs including warfarin and aspirin, and many other endogenous and exogenous compounds rely on albumin for transport and delivery. When albumin is low, the transport and bioavailability of these molecules is altered – which is why low albumin can affect everything from drug dosing accuracy to calcium interpretation to hormone function.
Why Albumin Matters for Performance and Longevity
For high performers, albumin matters both as a nutritional marker and as a longevity indicator. On the nutritional side, albumin reflects the adequacy of protein intake and absorption relative to the body’s demands. Intense training increases protein turnover, and sub-optimal albumin can indicate that dietary protein – despite seemingly adequate intake – is not meeting the demands of synthesis and recovery. For longevity, albumin is one of the most robust biomarkers associated with all-cause mortality in population studies: lower albumin within the “normal” range is consistently associated with worse outcomes across aging populations. This does not mean albumin causes aging – it reflects that the biological processes driving albumin down (inflammation, liver function decline, nutritional inadequacy) are the same processes driving health decline.
Albumin also directly affects how medications and hormones work. If albumin is low, the free (unbound) fraction of albumin-bound substances increases – potentially altering drug toxicity, hormone availability, and nutrient delivery. A low-normal albumin in someone on multiple medications or in someone trying to optimize testosterone or thyroid hormones may be affecting how those hormones function biologically regardless of what total serum levels show.
Normal vs. Optimal Albumin Levels
Standard Reference Ranges: Most laboratories report serum albumin as normal between 3.5 and 5.0 g/dL. Below 3.5 g/dL is hypoalbuminemia. This range identifies clinically significant albumin deficiency but is not optimized for performance or longevity.
The Problem With “Normal”: Albumin at 3.6 g/dL and 4.8 g/dL are both “normal.” They do not reflect the same biological reality. Multiple prospective studies show that albumin in the lower half of the reference range (3.5-4.0 g/dL) is associated with significantly higher all-cause mortality, hospitalization risk, and functional decline compared to albumin in the higher half (4.0-5.0 g/dL). The albumin trajectory over time – whether it is trending up or down over years of serial measurements – may be even more predictive than any single value. A progressive decline from 4.8 to 4.0 to 3.8 g/dL over years is a meaningful signal worth investigating, even though every individual value is “normal.”
Optimal Albumin for Longevity and Performance: For most healthy adults, albumin between 4.0 and 5.0 g/dL represents a well-maintained protein synthetic capacity and nutritional status. Albumin trending below 4.0 g/dL should prompt review of dietary protein intake, absorption adequacy, liver function, kidney protein losses (check urine protein), and inflammatory burden. For older adults, maintaining albumin above 4.0 g/dL is particularly important for muscle mass preservation, immune function, and functional independence.
What Causes Low Albumin?
Liver disease is the most clinically important cause – the liver is the sole source of albumin, and impaired hepatic function reduces albumin synthesis. Cirrhosis, severe hepatitis, and liver failure all cause declining albumin. Malnutrition and inadequate dietary protein are common causes globally and in hospitalized patients – when protein intake is insufficient, albumin synthesis falls as the liver prioritizes essential metabolic functions over protein production. Chronic inflammation dramatically suppresses albumin synthesis – albumin is a negative acute phase reactant, meaning the liver intentionally reduces albumin production during inflammatory states to redirect resources toward producing acute phase proteins like CRP and fibrinogen. This is why inflammatory and chronic disease states almost universally show lower albumin regardless of dietary intake. Nephrotic syndrome causes massive albumin losses through the kidneys – urine protein excretion can be several grams per day, rapidly depleting serum albumin. Protein-losing enteropathy from inflammatory bowel disease, celiac disease, or gut infections causes GI albumin losses. Hyperthyroidism increases albumin catabolism. Pregnancy naturally lowers albumin through hemodilution and increased catabolism.
What Causes High Albumin?
True hyperalbuminemia (albumin above 5.0 g/dL) is uncommon. The most common cause of apparently elevated albumin is dehydration – as plasma volume contracts, albumin concentration rises without any actual increase in albumin mass. In a well-hydrated person, albumin above 5.0 g/dL is rare and usually reflects a lab artifact or hemoconcentration. Unlike many biomarkers where higher is better within a range, there is no evidence that albumin above 5.0 g/dL confers additional benefit compared to 4.5 g/dL.
Albumin and Calcium: The Important Correction
Approximately 40% of serum calcium is bound to albumin. When albumin is low, total calcium appears falsely low even when ionized (free, biologically active) calcium is normal. This is clinically important: if you see low calcium on a panel alongside low albumin, the calcium is likely a mathematical consequence of low albumin rather than true hypocalcemia. The correction formula is: Corrected Calcium = Measured Calcium + 0.8 x (4.0 – Albumin). Using this formula corrects for the albumin effect and gives a more accurate picture of actual calcium status. When albumin is significantly low, directly measuring ionized calcium is more accurate than the correction formula.
Albumin and Hormone Optimization
Albumin binds sex hormone binding globulin (SHBG)-independent testosterone loosely, and this albumin-bound fraction is biologically active along with free testosterone. When albumin is low, the calculation of bioavailable testosterone (which includes both free and albumin-bound fractions) is affected. For people pursuing hormone optimization, low albumin can alter how testosterone distributes between bound and unbound fractions, affecting the accuracy of standard testosterone interpretation. Optimizing albumin through nutrition and reducing inflammatory burden is therefore part of the foundation for reliable hormone assessment and optimization.
Frequently Asked Questions
What albumin level is optimal for longevity?
Research consistently shows that albumin in the upper half of the reference range (above 4.0-4.2 g/dL) is associated with better long-term health outcomes, lower all-cause mortality, and better functional status in aging populations. There is no evidence of benefit from exceeding 5.0 g/dL. Maintaining albumin above 4.0 g/dL through adequate protein intake, liver health, controlled inflammation, and normal kidney function represents a meaningful longevity target.
Can I raise my albumin by eating more protein?
If albumin is low due to inadequate dietary protein intake or absorption, yes – improving protein intake (targeting 1.2-1.6 g/kg body weight daily for active adults) can raise albumin over weeks to months. If albumin is low due to liver disease, inflammation, or kidney protein losses, dietary protein alone will not be sufficient without addressing the underlying cause. Albumin reflects the balance between synthesis and losses, and both sides of that equation matter.
How quickly does albumin change?
Albumin has a half-life of approximately 20 days in the bloodstream, so it changes slowly. It takes 4-6 weeks to see meaningful changes in serum albumin from nutritional interventions or after resolution of acute illness. This slow response makes albumin a useful marker of sustained nutritional and hepatic status rather than acute changes. For monitoring rapid nutritional changes, prealbumin (transthyretin) with its 2-day half-life is more sensitive.
Does inflammation lower albumin?
Yes, significantly. Albumin is a negative acute phase reactant – during inflammatory states, the liver intentionally downregulates albumin production to redirect protein synthesis toward acute phase proteins like CRP, fibrinogen, and ferritin. This means that low albumin in the context of elevated CRP or other inflammatory markers may reflect inflammation rather than nutritional deficiency. Treating the underlying inflammatory burden – whether from autoimmune disease, chronic infection, metabolic syndrome, or lifestyle factors – is essential for albumin to recover.
Should albumin be checked alongside liver tests?
Yes. Albumin, total protein, and globulins are part of the liver function panel, complementing the liver enzyme tests (ALT, AST, ALP, bilirubin). Liver enzymes reflect liver cell damage. Albumin and total protein reflect liver synthetic function. It is possible to have elevated liver enzymes but normal synthetic function (acute injury without functional compromise) or normal liver enzymes with impaired synthetic function (chronic liver disease where cells have been replaced by scar tissue). The combination provides a more complete picture of liver health than either set of tests alone.
Testing Albumin With ApexBlood
Albumin is included in ApexBlood’s comprehensive panel alongside liver enzymes, kidney function markers, inflammatory indicators, and total protein – giving you the context to interpret what your albumin level actually means. A declining albumin trend alongside rising CRP tells a different story than declining albumin alongside rising urine protein. Our physicians interpret your complete picture to identify what is driving any albumin change and what the appropriate response is.
You cannot optimize what you do not measure. Albumin is one of the most informative longevity markers available – stop treating it as background noise on your panel.
Get comprehensive testing for $189
The Bottom Line on Albumin
Albumin is one of the most integrative biomarkers on your panel – it reflects your liver’s synthetic function, your nutritional adequacy, your inflammatory burden, and your kidney health all in a single number. The “normal” range extends from 3.5 to 5.0 g/dL, but optimal is consistently in the upper half, above 4.0 g/dL. A slow decline in albumin over years of serial testing – even while staying within the reference range – is a signal worth investigating, not dismissing. High performers understand that trends matter as much as single values. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Albumin and protein status require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.