
Alkaline phosphatase – ALP – is a liver and bone enzyme that gets far less attention than ALT or AST in discussions of liver health, yet it provides crucial diagnostic information that the other enzymes cannot. ALP is produced primarily in the liver (by bile duct cells), bone (by osteoblasts during bone formation), and to a lesser degree by the intestines, kidneys, and placenta. When ALP is elevated, the first clinical question is: is this coming from the liver or from bone? The answer changes everything about what the elevation means and what response is appropriate. For high performers, ALP in context with the complete liver panel and bone markers tells a story about both liver and bone health that deserves more than a cursory glance.
What Is Alkaline Phosphatase (ALP)?
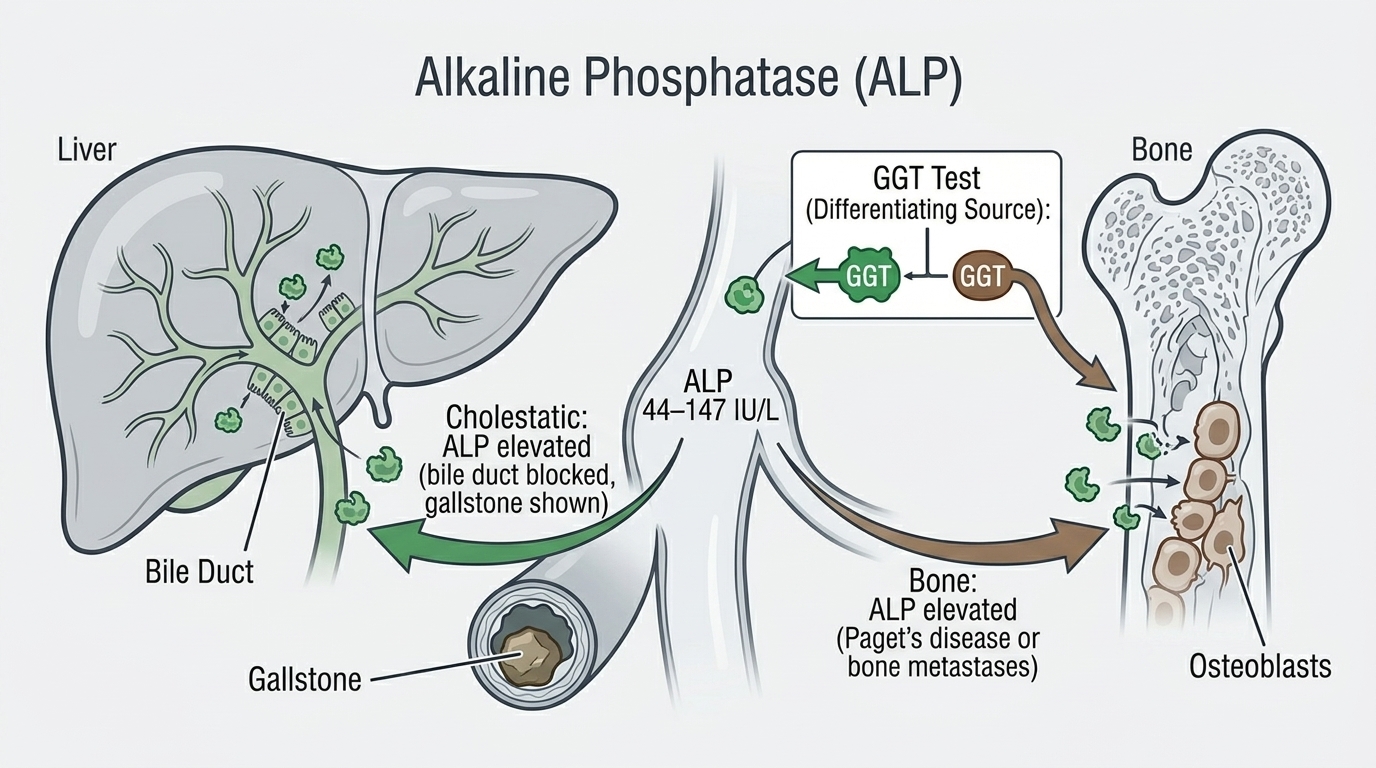
ALP is a hydrolase enzyme that removes phosphate groups from molecules – a reaction that occurs throughout the body but is particularly active in liver bile duct cells and bone-forming cells (osteoblasts). In the liver, ALP is concentrated in the cells lining the bile ducts and is released into the bloodstream when these ducts are under pressure from blocked bile flow, inflammation, or infiltrative disease. In bone, ALP is produced by osteoblasts as they build new bone tissue – so elevated bone ALP reflects active bone formation or bone disease.
Total ALP measured on standard blood panels is the sum of all isoforms – liver, bone, intestinal, and others. When ALP is elevated and the source is unclear, fractionation (measuring the specific ALP isoforms) or using accompanying markers (GGT to identify liver-specific ALP, bone-specific ALP for bone-related elevation) helps distinguish the source. GGT is particularly useful: if both ALP and GGT are elevated, liver disease is the likely source. If ALP is elevated but GGT is normal, bone disease or a physiological state (growth, pregnancy) is more likely.
Why ALP Matters for Performance and Health
ALP elevation – particularly liver-source ALP – is a hallmark of cholestasis: impaired bile flow. This can result from intrahepatic causes (inflammation, fatty liver disease, medication effects, primary biliary cholangitis) or extrahepatic causes (gallstones in the bile duct, pancreatic cancer compressing the bile duct, strictures). Identifying bile flow impairment early – before bilirubin rises to the point of jaundice – allows for earlier intervention and better outcomes. Non-alcoholic fatty liver disease (NAFLD), which affects 25-30% of Western adults, can elevate ALP alongside ALT as one of its early biochemical signatures. For anyone pursuing metabolic health optimization, an elevated ALP deserves investigation rather than dismissal.
Normal vs. Optimal ALP Levels
Standard Reference Ranges: Most laboratories report ALP as normal between 44 and 147 U/L for adults, though ranges vary by lab and differ significantly by age and sex. Children and adolescents have much higher ALP from active bone growth (often 2-5x adult values). Pregnant women in the third trimester have elevated ALP from placental production. These physiological elevations are normal and expected.
The Problem With “Normal”: ALP at 50 U/L and 140 U/L are both “normal,” but they do not reflect the same liver health state. A rising ALP trend toward the upper end of normal – even before it exceeds the reference range – may indicate developing cholestatic liver disease or progressive bone disease that benefits from early identification. For adults on no medications and without active bone growth, ALP consistently above 100-120 U/L warrants checking GGT and reviewing medications, alcohol intake, and liver ultrasound if the trend continues.
Optimal ALP: For most healthy adults, ALP in the range of 50-100 U/L with normal GGT and other liver markers suggests healthy bile duct function. Low ALP (below 40 U/L) can occur with hypothyroidism, zinc deficiency, pernicious anemia, or cardiac surgery with bypass, and while less commonly discussed, deserves investigation if persistent.
What Causes Elevated ALP?
Liver causes of elevated ALP include bile duct obstruction from gallstones or tumors (which produces the highest ALP values, sometimes 10-20x normal), primary biliary cholangitis (an autoimmune bile duct disease), primary sclerosing cholangitis, drug-induced cholestasis (common culprits include anabolic steroids, oral contraceptives, some antibiotics, and statins), non-alcoholic fatty liver disease, and infiltrative liver diseases including sarcoidosis and liver metastases. Bone causes of elevated ALP include Paget’s disease of bone, bone metastases from cancer, hyperparathyroidism causing bone resorption, healing fractures, and osteomalacia (vitamin D deficiency causing softened bones with active osteoblastic response). Physiological elevations occur during growth, pregnancy, and occasionally following a high-fat meal (intestinal ALP transient elevation).
Frequently Asked Questions
How do I know if elevated ALP is from liver or bone?
GGT (gamma-glutamyl transferase) is the most practical clinical tool for this distinction. GGT is elevated in liver disease but not in bone disease. If both ALP and GGT are elevated, the ALP is liver-sourced. If ALP is elevated but GGT is normal, bone disease or a physiological state (growth, pregnancy) is the likely source. Bone-specific ALP testing and bone markers (like bone alkaline phosphatase, P1NP) can provide further confirmation when needed.
Can medications cause elevated ALP?
Yes – several commonly used medications cause cholestatic liver injury with elevated ALP as the primary finding. Anabolic steroids (including some that appear in supplements), oral contraceptives, some antibiotics (amoxicillin-clavulanate, fluoroquinolones), phenothiazines, and some antifungal medications can all cause cholestatic ALP elevation. If ALP is elevated and you are on any regular medications or supplements, a medication review should be part of the workup.
Is low ALP a concern?
Low ALP (below 40 U/L) is less commonly discussed but can indicate hypothyroidism, zinc deficiency, pernicious anemia (B12 deficiency), or hypophosphatasia – a rare genetic condition causing impaired bone and dental development. If ALP is consistently low without an obvious explanation, thyroid function and zinc status are reasonable first-line investigations.
Testing ALP With ApexBlood
ALP is included in ApexBlood’s comprehensive liver function panel alongside ALT, AST, bilirubin, albumin, and GGT – giving you the complete liver and bile duct health picture. ALP in context with GGT and other liver markers provides the information needed to distinguish cholestatic from hepatocellular patterns of liver injury and identify the most appropriate next steps.
Get comprehensive testing for $189
The Bottom Line on ALP
ALP is the bile duct and bone enzyme that tells you whether something is impeding bile flow or disrupting bone metabolism. A rising ALP – even within the reference range – alongside elevated GGT is a signal to investigate your liver health proactively. An elevated ALP with normal GGT directs investigation toward bone. Neither pattern should be dismissed without understanding the underlying cause. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. ALP and liver/bone health require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.