
AST – aspartate aminotransferase – is a liver enzyme that appears on every standard metabolic panel, yet most people who receive their results have little understanding of what it actually measures, what elevates it, or what an abnormal value means for their health. AST is an enzyme found inside liver cells (and muscle cells, heart cells, and red blood cells), and it leaks into the bloodstream when these cells are damaged or destroyed. Unlike ALT (which is more liver-specific), AST elevation can come from the heart, skeletal muscle, or red blood cells – which makes the AST/ALT ratio clinically important for understanding what type of injury is occurring. Understanding your AST in context is the difference between identifying a liver problem early and missing muscle damage that has an entirely different cause and response.
What Is AST?
Aspartate aminotransferase (AST, also called SGOT – serum glutamic-oxaloacetic transaminase in older terminology) is an enzyme that facilitates the transfer of amino groups in amino acid metabolism. It is found in the cytoplasm and mitochondria of cells, with the highest concentrations in the liver, cardiac muscle, skeletal muscle, kidneys, brain, and red blood cells. When any of these cells are damaged – by inflammation, injury, toxins, or ischemia – AST leaks out of the intracellular environment into the bloodstream, where it can be measured.
AST has a half-life of approximately 17 hours in the bloodstream – shorter than ALT (which has a half-life of 47 hours). This means AST rises and falls more quickly after an acute injury event. After a heart attack, for example, AST rises within 6-12 hours, peaks at 24-48 hours, and normalizes within 3-5 days. After strenuous exercise that damages muscle cells, AST can rise significantly within hours and return toward normal within 2-5 days. Understanding the timing of any AST elevation relative to symptoms and activities is essential context for interpretation.
Why AST Matters for Performance and Liver Health
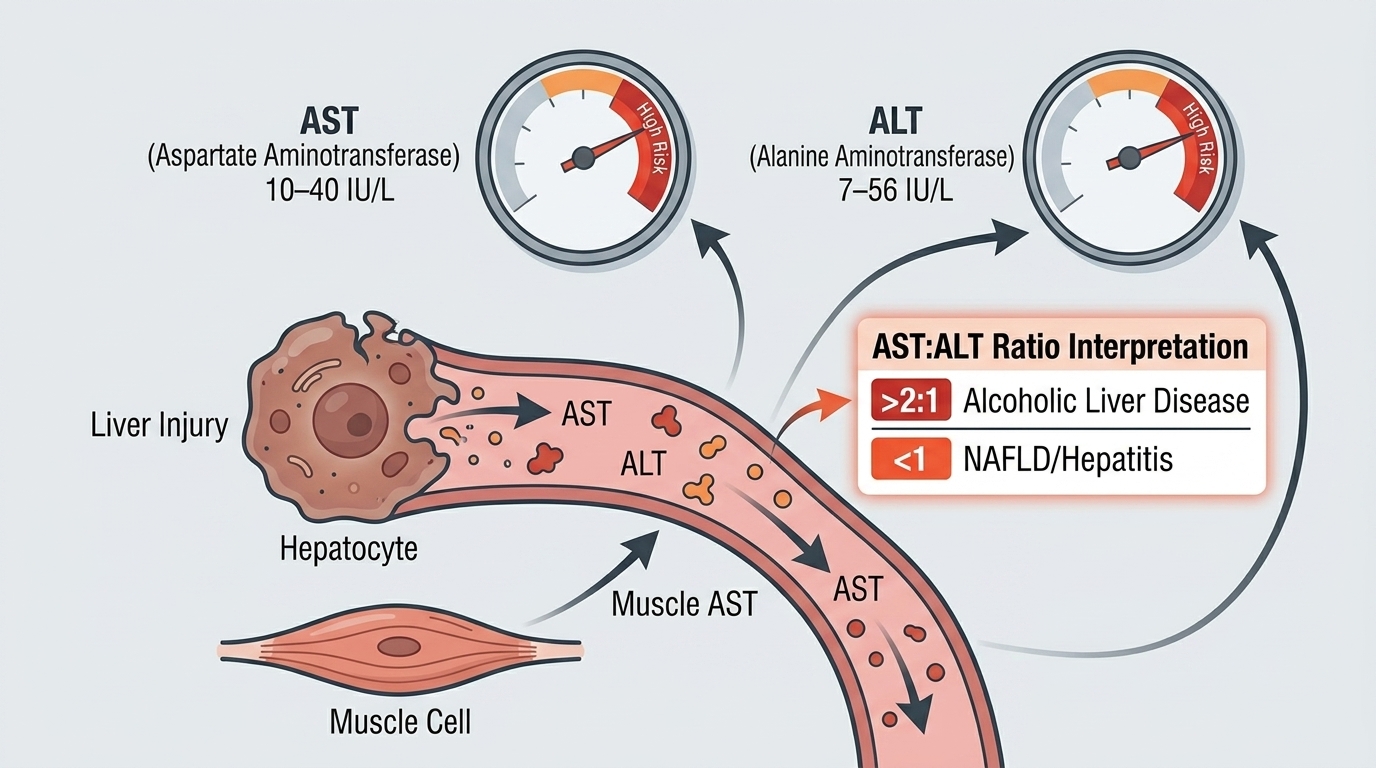
For most healthy people, AST is primarily valuable as a liver health indicator in combination with ALT. Together, they assess hepatocellular (liver cell) injury. Elevated AST alongside elevated ALT points toward liver injury – from fatty liver disease, hepatitis, alcohol damage, or medication effects. The ratio of AST to ALT (the De Ritis ratio) provides additional diagnostic information: an AST/ALT ratio above 2:1 is classically associated with alcoholic liver disease, while ratios below 1:1 (ALT higher than AST) more typically reflect non-alcoholic fatty liver disease or viral hepatitis.
For athletes, AST is particularly important to contextualize carefully. Strenuous exercise – particularly resistance training, endurance running, or any activity causing significant muscle stress – routinely elevates AST from skeletal muscle damage, not liver damage. An athlete who tests within 24-48 hours of a hard training session may show AST values 2-4x the upper limit of normal with a completely healthy liver. The clinical error of misinterpreting exercise-induced AST elevation as liver disease is common. The key distinguisher is ALT – exercise elevates AST much more than ALT, while liver disease elevates both. If AST is elevated with a normal ALT, skeletal muscle is the likely source. If both are elevated proportionally, liver investigation is warranted.
Normal vs. Optimal AST Levels
Standard Reference Ranges: Most laboratories report AST as normal between 10 and 40 U/L for adults, with some labs setting the upper limit slightly higher (up to 50 U/L). These ranges are established from population studies and are designed to identify significant hepatocellular or muscle injury. Mild elevations (40-100 U/L) may have benign causes including recent exercise. Moderate elevations (100-300 U/L) warrant investigation. Severe elevations (above 1,000 U/L) indicate acute severe injury – from acute hepatitis, ischemic hepatitis (“shock liver”), drug-induced liver injury, or massive muscle trauma (rhabdomyolysis).
The Importance of Context: AST is one of the biomarkers where a single value in isolation is genuinely difficult to interpret. Was blood drawn within 48 hours of intense exercise? Has there been recent alcohol consumption? Are there medications or supplements that might affect the liver? Is ALT also elevated? Without this context, an elevated AST cannot be accurately interpreted. The AST/ALT ratio, the absolute magnitude, the trajectory over time, and accompanying markers (ALP, bilirubin, albumin) together tell the complete story.
Optimal AST for Liver Health: For sedentary or moderately active adults without recent strenuous exercise, AST below 30 U/L with normal ALT suggests healthy hepatocellular integrity. Some functional medicine practitioners argue that optimal is below 25 U/L, particularly in the context of optimizing metabolic health and minimizing subclinical liver inflammation. For athletes, allowing 48-72 hours after heavy training before interpreting liver enzymes gives a cleaner baseline.
What Causes Elevated AST?
Liver causes include non-alcoholic fatty liver disease (NAFLD – the most common cause of mildly elevated AST in the outpatient setting), alcoholic liver disease (often with AST/ALT ratio above 2:1), viral hepatitis (A, B, C), autoimmune hepatitis, drug-induced liver injury (common culprits include acetaminophen, statins, antibiotics, herbal supplements), and cirrhosis. Non-liver causes include vigorous exercise (skeletal muscle AST release – often with elevated CK), rhabdomyolysis (severe muscle breakdown causing dramatically elevated AST and CK alongside kidney injury risk), cardiac muscle injury (heart attack was historically diagnosed partly with AST elevation before troponin replaced it), hemolysis (red blood cells contain AST and release it when destroyed), and thyroid disease (hypothyroidism can mildly elevate AST through uncertain mechanisms). The co-elevation of CK (creatine kinase) alongside AST with a normal ALT points strongly toward muscle rather than liver as the source.
The AST/ALT Ratio: A Powerful Diagnostic Tool
The ratio of AST to ALT (De Ritis ratio) provides meaningful additional diagnostic information. AST/ALT below 1 (ALT higher) is typical of viral hepatitis and non-alcoholic fatty liver disease. AST/ALT above 2:1 is the classic pattern of alcoholic liver disease – the mitochondrial form of AST is selectively elevated by alcohol. AST/ALT above 3:1 strongly suggests alcoholic hepatitis. Exercise-induced elevation typically shows AST/ALT ratios well above 2:1 because skeletal muscle contains much more AST than ALT. Cirrhosis from any cause often progresses to AST/ALT ratios above 1 as the liver loses its ALT-producing hepatocytes.
Frequently Asked Questions
Can exercise cause high AST?
Yes – significantly. Strenuous exercise, particularly resistance training and endurance running, causes skeletal muscle cell damage that releases AST into the bloodstream. AST can rise 2-10x above normal within 24-48 hours of a hard training session. This is entirely normal exercise physiology, not liver disease. If AST is elevated after exercise, check CK (creatine kinase) – if CK is also elevated with a normal ALT, muscle is the source. If ALT is also elevated with AST, liver investigation is warranted.
Is AST or ALT a better liver test?
ALT is more liver-specific than AST because it is found in lower concentrations in skeletal muscle, heart, and other non-liver tissues. This makes ALT the preferred single marker for liver health screening. However, the combination of both – and particularly the AST/ALT ratio – provides more diagnostic information than either alone. The ratio helps distinguish alcoholic liver disease (high ratio) from NAFLD and hepatitis (low ratio) and exercise-induced elevation (high ratio with high CK).
What supplements or medications commonly elevate AST?
Acetaminophen (Tylenol) at high doses or in combination with alcohol is a leading cause of drug-induced liver injury with dramatic AST elevation. Herbal supplements including kava, valerian, comfrey, certain traditional Chinese medicines, and some gym supplements can cause hepatotoxicity. Statins can mildly elevate liver enzymes in some people. Anabolic steroids (including those found in some “natural” sports supplements) commonly elevate AST. If AST is elevated and you are on any regular medications or taking supplements, a thorough review is essential.
How long does it take elevated AST to normalize?
AST has a shorter half-life than ALT (approximately 17 hours versus 47 hours), so it normalizes faster after an acute injury. Exercise-induced AST typically peaks 24-48 hours post-exercise and normalizes within 3-5 days. After acute viral hepatitis, AST may take weeks to months to normalize. After stopping an offending medication causing drug-induced liver injury, AST typically normalizes within weeks to months depending on the severity of injury and the specific drug involved.
Testing AST With ApexBlood
AST is included in ApexBlood’s comprehensive liver function panel alongside ALT, ALP, bilirubin, albumin, and GGT. The complete panel allows accurate interpretation of the pattern – hepatocellular versus cholestatic, alcoholic versus non-alcoholic, liver versus muscle source. If AST is elevated on your panel, our physicians can discuss the likely causes based on your complete picture and lifestyle context, and recommend appropriate follow-up rather than leaving you with an unexplained number.
Get comprehensive testing for $189
The Bottom Line on AST
AST is a liver and muscle enzyme that requires context to interpret accurately. Elevated AST from exercise is a normal physiological response. Elevated AST from liver disease is a signal requiring investigation and action. The AST/ALT ratio, the presence or absence of CK elevation, and the complete liver panel together tell the story that a single AST value cannot. For high performers who train hard and care about liver health, drawing blood 48-72 hours away from intense exercise gives the cleanest baseline. Stop accepting an unexplained elevated AST as “something to watch” without understanding what is driving it. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. AST and liver health require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.