
Bilirubin is a yellow-orange pigment produced when your body breaks down old red blood cells, and it is one of the most informative markers on a liver function panel. Most people know bilirubin as the substance that turns skin and eyes yellow in jaundice – but by that point, bilirubin is dramatically elevated. The more practically relevant question is what your bilirubin level reveals before it reaches that stage: about your liver’s ability to process waste products, your rate of red blood cell breakdown, the health of your bile ducts, and – perhaps surprisingly – your cardiovascular and metabolic health. A mildly elevated bilirubin in a healthy young person often signals nothing alarming. A persistently low-normal bilirubin in someone with liver disease may not be reassuring. Understanding what your bilirubin actually means requires the context of the full liver panel and an understanding of how bilirubin is produced, processed, and excreted.
What Is Bilirubin?
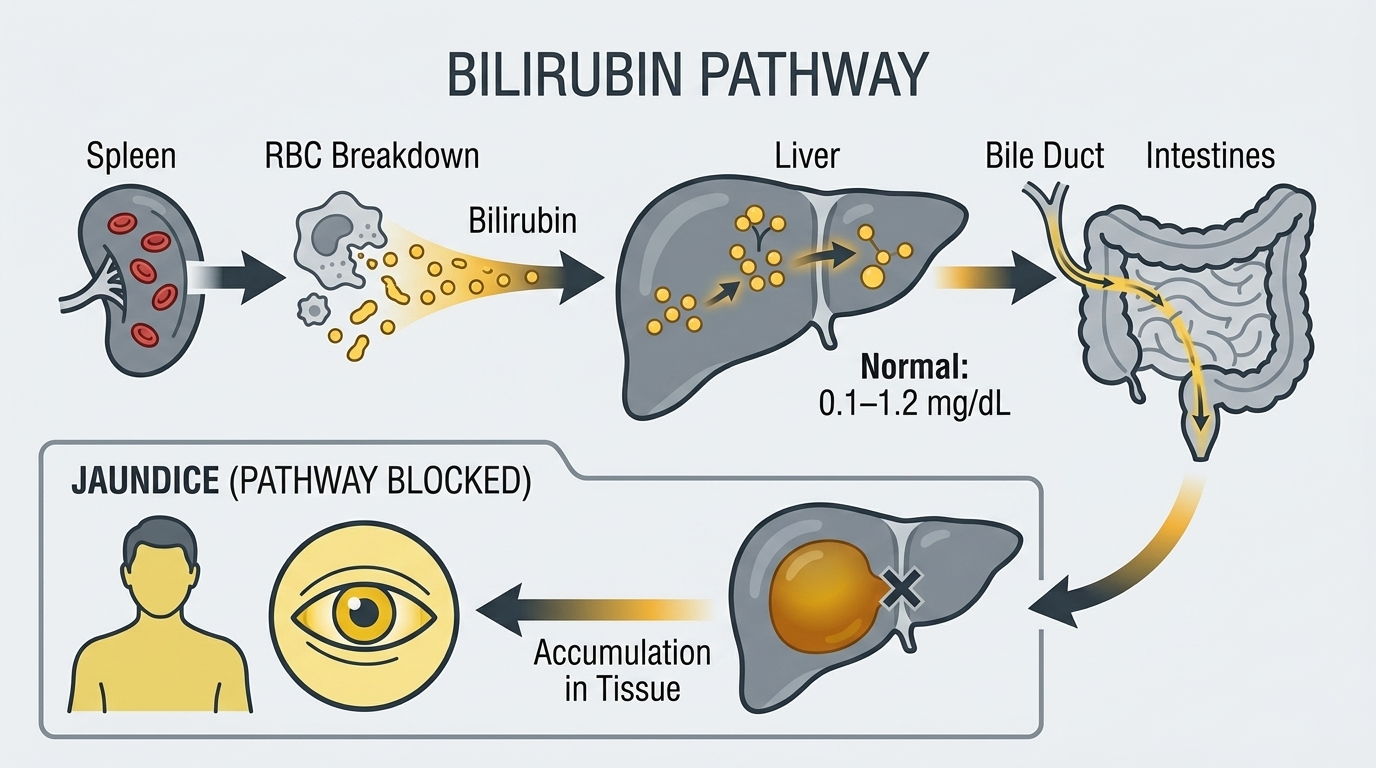
Bilirubin is produced from the breakdown of heme – the iron-containing component of hemoglobin in red blood cells. When red blood cells reach the end of their approximately 120-day lifespan, they are destroyed by macrophages in the spleen and liver, releasing hemoglobin. The heme portion is converted to biliverdin and then to bilirubin in the tissues, producing what is called unconjugated (indirect) bilirubin – which is fat-soluble and bound to albumin in the bloodstream.
The liver then picks up this unconjugated bilirubin, attaches glucose molecules to make it water-soluble through a process called conjugation, and excretes it into bile. This conjugated (direct) bilirubin flows through bile ducts into the intestines, where gut bacteria convert it to urobilinogen – some of which is reabsorbed and excreted in urine (giving urine its yellow color), and some of which is converted to stercobilin and excreted in stool (giving stool its brown color). A standard bilirubin test reports total bilirubin (direct plus indirect) and often direct bilirubin separately – from which indirect bilirubin can be calculated.
Why Bilirubin Matters for Health and Longevity
Bilirubin is primarily a liver and bile duct health marker. The liver’s ability to take up, conjugate, and excrete bilirubin reflects its functional reserve – how well it is performing one of its core detoxification and elimination tasks. Elevated bilirubin indicates either that the liver is overwhelmed (from excessive red blood cell breakdown or liver disease impairing processing), or that bile cannot flow normally from the liver to the intestines (obstruction from gallstones, tumors, or bile duct disease).
Beyond liver health, bilirubin has a genuinely interesting relationship with cardiovascular and metabolic health. Bilirubin is a potent antioxidant – it scavenges free radicals and inhibits LDL cholesterol oxidation. Multiple large population studies show that people with higher bilirubin within the normal range have lower rates of cardiovascular disease, metabolic syndrome, and certain cancers. This has generated interest in whether mildly elevated bilirubin (as seen in Gilbert syndrome, discussed below) is actually protective rather than pathological. Understanding the mechanism – and whether it translates to interventional benefit – remains an active area of research.
Normal vs. Optimal Bilirubin Levels
Standard Reference Ranges: Total bilirubin is reported as normal between 0.2 and 1.2 mg/dL in most laboratories. Direct (conjugated) bilirubin is normally below 0.3 mg/dL. Jaundice becomes clinically visible when total bilirubin exceeds approximately 2.5-3.0 mg/dL. These ranges reliably identify significant abnormalities. Mild elevations between 1.2 and 2.0 mg/dL without other liver enzyme abnormalities often reflect Gilbert syndrome – a benign genetic variant affecting bilirubin conjugation enzymes – rather than liver disease.
The Nuance of “Normal” Bilirubin: Unlike many biomarkers where the upper end of normal is the concern, bilirubin’s relationship with health is more complex. Higher bilirubin within the normal range (0.6-1.2 mg/dL) has been associated in observational studies with lower cardiovascular risk, better antioxidant status, and lower metabolic disease rates. Lower bilirubin (below 0.4 mg/dL) has been associated with higher oxidative stress and potentially higher cardiovascular risk in some analyses. This does not mean you should try to raise your bilirubin – it is largely genetically determined – but it does mean that mildly elevated bilirubin in an otherwise healthy person with normal liver enzymes is often benign or even favorable.
What Causes High Bilirubin?
Elevated bilirubin has three mechanistic categories that point toward completely different conditions. Pre-hepatic (before the liver) causes involve excessive red blood cell destruction producing more bilirubin than the liver can process. Hemolytic anemias – from autoimmune hemolysis, sickle cell disease, G6PD deficiency, hereditary spherocytosis, or transfusion reactions – cause elevated indirect (unconjugated) bilirubin with normal liver enzymes. Hepatic (liver) causes impair the liver’s ability to take up, conjugate, or secrete bilirubin. Gilbert syndrome – the most common hereditary disorder of bilirubin metabolism, affecting 3-7% of the population – causes mildly elevated indirect bilirubin (typically 1.2-3.0 mg/dL) due to reduced UDP-glucuronosyltransferase enzyme activity. It is benign and often triggered by fasting, stress, or illness. Liver diseases including hepatitis (viral, alcoholic, or autoimmune), cirrhosis, and drug-induced liver injury impair bilirubin processing and cause elevated direct and/or indirect bilirubin alongside elevated liver enzymes. Post-hepatic (after the liver) causes involve blockage of bile flow – gallstones in the bile duct, pancreatic cancer compressing the bile duct, cholangiocarcinoma, or strictures. These cause elevated direct (conjugated) bilirubin because the liver has conjugated bilirubin normally but cannot excrete it into the intestines. This pattern requires urgent investigation.
Gilbert Syndrome: The Common “Non-Disease”
Gilbert syndrome deserves special mention because it is extremely common (3-7% of the population) and frequently causes unnecessary concern when discovered on routine blood work. People with Gilbert syndrome have a genetic variant that reduces the activity of the enzyme that conjugates bilirubin, resulting in mildly elevated unconjugated bilirubin – typically between 1.2 and 3.0 mg/dL, fluctuating with fasting, illness, dehydration, and stress. It requires no treatment, causes no long-term liver damage, and is considered by most researchers to be a benign variant or even potentially protective given the antioxidant properties of bilirubin. Suspecting Gilbert syndrome versus liver disease requires checking that direct bilirubin is normal (below 0.3 mg/dL) and that ALT, AST, ALP, and albumin are all normal. If all other liver markers are normal and only unconjugated bilirubin is mildly elevated, Gilbert syndrome is the most likely explanation.
Frequently Asked Questions
Is mildly elevated bilirubin always dangerous?
No. Mildly elevated total bilirubin (1.2-3.0 mg/dL) with normal direct bilirubin and normal liver enzymes (ALT, AST, ALP) in an otherwise healthy person is usually Gilbert syndrome – a benign genetic variant affecting 3-7% of people. It requires no treatment and is not associated with liver damage. Elevated direct bilirubin or elevated bilirubin alongside abnormal liver enzymes is more concerning and warrants investigation.
What is the difference between direct and indirect bilirubin?
Indirect (unconjugated) bilirubin is the fat-soluble form produced from red blood cell breakdown, circulating bound to albumin before the liver processes it. Direct (conjugated) bilirubin is the water-soluble form that the liver has processed and is ready to excrete in bile. High indirect bilirubin (with normal direct) suggests either excessive red blood cell breakdown or impaired liver uptake and conjugation (as in Gilbert syndrome). High direct bilirubin suggests the liver has processed bilirubin but cannot excrete it properly – indicating bile duct obstruction or severe hepatocellular disease.
Can jaundice occur with normal bilirubin?
No. Jaundice (yellowing of the skin and whites of the eyes) requires bilirubin to be elevated above approximately 2.5-3.0 mg/dL. If you see yellowing below this threshold, it may be carotenemia (excess beta-carotene from diet causing skin yellowing without eye involvement) rather than true jaundice. True jaundice always reflects significantly elevated bilirubin.
Does fasting affect bilirubin?
Yes – significantly in people with Gilbert syndrome. Fasting for 24-48 hours can raise bilirubin by 2-3x in individuals with Gilbert syndrome. This is why bilirubin on a blood test drawn after an overnight fast may be higher than a random draw, and why illness, stress, and strenuous exercise (which create mild metabolic stress similar to fasting) temporarily elevate bilirubin in people with this genetic variant.
Is high bilirubin protective against heart disease?
Observational data consistently shows lower cardiovascular disease rates in people with higher bilirubin levels within the normal range, including those with Gilbert syndrome. Bilirubin is a potent antioxidant that inhibits LDL oxidation and may reduce vascular inflammation. However, this association does not prove causation, and there is no evidence that artificially raising bilirubin provides cardiovascular benefit. It does suggest that mildly elevated bilirubin in an otherwise healthy person should not be aggressively treated.
Testing Bilirubin With ApexBlood
Bilirubin is included in ApexBlood’s comprehensive liver function panel alongside ALT, AST, ALP, albumin, and total protein – giving you the complete picture of liver synthetic function, liver cell health, and bile flow. Any bilirubin elevation can be properly contextualized alongside these markers to distinguish Gilbert syndrome from liver disease from bile duct obstruction. Our physicians interpret your complete liver panel rather than reacting to individual numbers in isolation.
Get comprehensive testing for $189
The Bottom Line on Bilirubin
Bilirubin is the most visible of the liver markers – when severely elevated, it turns you yellow. But the clinically relevant questions are usually subtler: is a mildly elevated bilirubin Gilbert syndrome (benign, common, possibly even cardioprotective) or the first sign of liver disease or bile duct obstruction? The answer lies in the complete liver panel, not the bilirubin number alone. Elevated direct bilirubin or bilirubin alongside elevated liver enzymes requires investigation. Isolated mildly elevated indirect bilirubin with a normal rest of the panel usually requires reassurance, not treatment. Stop accepting “your bilirubin is a little elevated, something to watch” without understanding what is actually going on. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Bilirubin and liver function require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.