
Calcium is the most abundant mineral in your body, and it is also one of the most tightly regulated. Your serum calcium level stays within a narrow band under virtually all circumstances – your body will strip calcium from your bones to maintain blood levels if dietary intake is inadequate. This tight regulation means that serum calcium is not a reliable indicator of your total body calcium status. But when serum calcium does fall outside the normal range, it signals something significant: either a problem with the regulatory systems themselves – your parathyroid glands, kidneys, or vitamin D metabolism – or occasionally an early signal of cancer or other serious disease. Understanding what your calcium level actually means requires understanding the whole regulatory system, not just the number on your lab report.
What Is Serum Calcium?
Calcium in your blood exists in three forms. About 40% is bound to albumin (a blood protein) and is inactive. About 10% is complexed with other ions like phosphate and citrate. The remaining 50% is ionized (free) calcium, which is the biologically active form that actually drives cellular functions. Standard blood panels report total calcium – the sum of all three forms. When albumin is low (from malnutrition, liver disease, or kidney disease), total calcium appears falsely low even when ionized calcium is normal. This is why albumin-corrected calcium or direct ionized calcium measurement provides a more accurate picture in people with abnormal albumin levels.
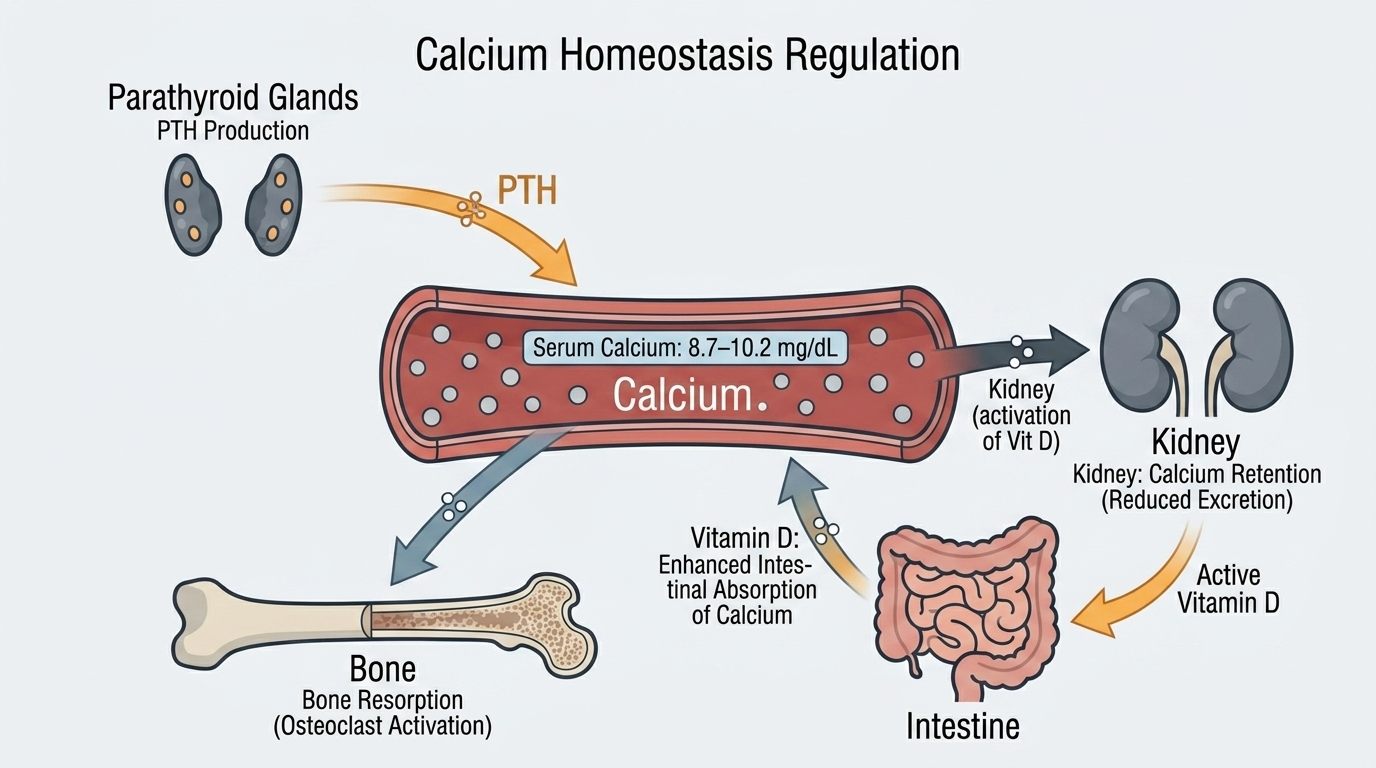
Calcium’s roles in your body extend far beyond bone structure: muscle contraction (including cardiac muscle), nerve signal transmission, blood clotting, hormone secretion, enzyme activation, and cell-to-cell communication all require calcium. The tight serum calcium regulation – maintained by parathyroid hormone (PTH), vitamin D, and calcitonin acting on the bones, kidneys, and gut – reflects how critical it is to keep this ion within a precise operating range.
Why Calcium Matters Beyond Bone Health
Most people think of calcium as a bone mineral, and it is – 99% of your body’s calcium is stored in bones and teeth, where it provides structural integrity. But the 1% in your bloodstream and cells is where calcium drives moment-to-moment physiology. Every heartbeat requires calcium. Every muscle contraction – from your diaphragm moving with each breath to your legs powering through a training session – is initiated by calcium ions flowing into muscle cells. Nerve impulses propagate via calcium-dependent mechanisms. Blood clotting cannot proceed without adequate calcium. Insulin secretion from the pancreas is calcium-dependent.
For high performers, calcium dysregulation – even subtle dysregulation within the “normal” range – affects muscle function, cardiac rhythm, neuromuscular performance, and recovery. The goal is not just to avoid deficiency but to maintain the regulatory systems – PTH, vitamin D, magnesium – that keep calcium optimally distributed between blood, bone, and cells.
Normal vs. Optimal Calcium Levels
Standard Reference Ranges: Most laboratories report total serum calcium as normal between 8.5 and 10.5 mg/dL (or 2.1-2.6 mmol/L). These ranges are well-established and clinically validated. Unlike many other biomarker reference ranges, calcium’s tight physiological regulation means that values consistently outside this range genuinely indicate a problem rather than simple population variation.
The Problem With “Normal”: Because calcium is so tightly regulated, a “normal” total calcium does not mean your calcium metabolism is optimal. It means the regulatory system is working hard enough to maintain serum levels. If you are chronically low in vitamin D or magnesium (both essential for calcium metabolism), your PTH may be chronically elevated to pull calcium from bones and maintain serum levels – protecting your blood calcium while slowly depleting your skeletal calcium reserves. Serum calcium looks fine. Bone density is quietly declining. The number alone does not tell that story.
Optimal Total Calcium: For most adults, total calcium between 9.0 and 10.2 mg/dL suggests healthy calcium metabolism and adequate regulatory function. Values consistently at the lower end of “normal” (8.5-9.0 mg/dL) alongside elevated PTH and low vitamin D should prompt investigation of the underlying regulatory issue rather than calcium supplementation alone. Values at the upper end of normal (above 10.2 mg/dL) without a clear cause warrant investigation to rule out hyperparathyroidism and hypercalcemia of malignancy.
What Causes High Calcium (Hypercalcemia)?
Primary hyperparathyroidism – usually caused by a benign tumor (adenoma) of one or more parathyroid glands – accounts for the majority of outpatient hypercalcemia cases. The abnormal parathyroid gland secretes excessive PTH regardless of calcium levels, continuously pulling calcium from bones into the bloodstream. Symptoms of mild hypercalcemia are notoriously vague: fatigue, cognitive dulling, constipation, increased urination, and mild depression. The classic teaching is “bones, stones, groans, and psychic moans” – bone loss, kidney stones, abdominal pain, and neuropsychiatric symptoms in more severe cases. Malignancy (cancer) is the second most common cause of elevated calcium, particularly in hospitalized patients – certain cancers produce PTH-related protein that mimics PTH action, and bone metastases release calcium directly from bone destruction. Excessive vitamin D supplementation, granulomatous diseases like sarcoidosis, and milk-alkali syndrome from excessive calcium supplementation can also cause hypercalcemia. Any calcium above 10.5 mg/dL consistently deserves investigation – this is not a case where “high normal” can be comfortably ignored.
What Causes Low Calcium (Hypocalcemia)?
Hypoparathyroidism – insufficient PTH production, most commonly following accidental damage to the parathyroid glands during thyroid surgery – is a major cause of chronically low calcium. Vitamin D deficiency is extremely common and impairs calcium absorption from the gut, eventually leading to hypocalcemia despite adequate dietary intake. Severe magnesium deficiency can cause hypocalcemia because magnesium is required for normal PTH secretion and for PTH to act properly on its target tissues. Kidney disease impairs the activation of vitamin D and can cause chronic hypocalcemia. Pseudohypoparathyroidism (resistance to PTH action) produces low calcium despite high PTH. Low albumin produces apparent hypocalcemia that corrects when albumin-adjusted calcium is calculated. Acute pancreatitis, massive blood transfusions, and some medications can also lower calcium acutely.
How to Support Optimal Calcium Metabolism
Optimizing calcium metabolism is about more than taking calcium supplements. The full regulatory system – vitamin D, magnesium, PTH, and kidney function – needs to work together for calcium to be properly absorbed, distributed, and used. Vitamin D (ideally 25-OH vitamin D between 40-60 ng/mL) is essential for calcium absorption from the gut – without adequate vitamin D, only 10-15% of dietary calcium is absorbed. Magnesium is essential for PTH secretion and PTH receptor function – without adequate magnesium, the calcium regulatory system cannot function properly even when calcium intake is sufficient. Vitamin K2 helps direct calcium to bones and teeth rather than soft tissues and arteries – important when supplementing calcium to prevent arterial calcification. Dietary calcium from dairy, leafy greens, sardines, and fortified foods is preferable to high-dose supplementation for most people. Excess supplemental calcium (above 1,000-1,200 mg per day from supplements) has been associated in some studies with increased cardiovascular risk, likely because of arterial calcium deposition.
Frequently Asked Questions
Does a normal serum calcium mean my calcium status is fine?
Not necessarily. Because serum calcium is so tightly regulated, your body will pull calcium from bones to maintain blood levels when intake or absorption is inadequate. Normal serum calcium alongside low vitamin D, elevated PTH, and poor dietary calcium intake means the regulatory system is working hard to maintain that normal number – possibly at the expense of bone density. The full context matters.
Should I be concerned if my calcium is slightly above normal?
Yes – consistently elevated calcium (above 10.5 mg/dL) should be investigated, not watched and waited. The two most common causes are primary hyperparathyroidism and malignancy, both of which benefit from early identification. A single borderline elevation may be a lab variation, but repeat elevations warrant PTH measurement and physician evaluation. Do not dismiss persistently high calcium as “just a little elevated.”
How much calcium do I actually need?
Most adults need 1,000-1,200 mg of calcium daily from all sources combined (food plus supplements). Dietary calcium from whole foods is preferable because it comes packaged with other nutrients that support absorption. If supplementing, divide doses (calcium is best absorbed in amounts under 500 mg at a time) and pair with vitamin D. Avoid supplementing more than 500-600 mg per dose and more than 1,000-1,200 mg total per day from supplements – excess has not been shown to benefit bone density and may increase cardiovascular risk.
How does vitamin D affect calcium?
Vitamin D is essential for calcium absorption in the gut. With adequate vitamin D (25-OH vitamin D above 30-40 ng/mL), roughly 30-40% of dietary calcium is absorbed. With vitamin D deficiency (below 20 ng/mL), absorption falls to 10-15%. This means that even a calcium-rich diet will not maintain calcium balance if vitamin D is deficient. Checking vitamin D alongside calcium is essential for understanding your calcium metabolism fully.
Can high calcium supplements cause problems?
Yes. Several large studies have associated high-dose supplemental calcium (particularly carbonate supplements above 1,000 mg/day) with increased risk of kidney stones and, in some analyses, increased cardiovascular events – potentially because calcium is depositing in arterial walls rather than bones. Taking vitamin K2 alongside calcium supplementation helps direct calcium to bone. Dietary calcium does not carry the same risks. Always discuss supplementation amounts with a physician, particularly if you have a history of kidney stones or cardiovascular disease.
What other tests should be done alongside calcium?
For a complete picture of calcium metabolism, the most valuable accompanying tests are PTH (parathyroid hormone), 25-OH vitamin D, magnesium, phosphate, and albumin (to correct for protein-binding effects on total calcium). If calcium is elevated, PTH measurement distinguishes between PTH-dependent causes (hyperparathyroidism) and PTH-independent causes (malignancy, excess vitamin D). If calcium is low, PTH helps distinguish between hypoparathyroidism and vitamin D deficiency as the underlying driver.
Testing Calcium With ApexBlood
Calcium is included in ApexBlood’s comprehensive blood panel alongside vitamin D, magnesium, phosphate, albumin, and kidney function markers that provide the full regulatory context. A calcium number in isolation tells you whether you are in range – but understanding your complete calcium metabolism requires seeing how your vitamin D, PTH (available through our physician-ordered custom panels), and magnesium are interacting with your calcium level.
You cannot optimize what you do not measure. Understanding your complete mineral metabolism gives you the precision to support bone health, cardiovascular function, and neuromuscular performance intelligently.
Get comprehensive testing for $189
The Bottom Line on Calcium
Serum calcium is tightly regulated, which means a normal value does not guarantee optimal calcium metabolism – it may just mean your regulatory systems are working hard to maintain appearances. When calcium falls outside the normal range, it signals a problem with the regulatory system itself that deserves investigation rather than a simple supplement recommendation. The most important questions are not just “what is your calcium?” but “what is your vitamin D, your PTH, and your magnesium?” – because those are what actually determine whether calcium is being properly absorbed, distributed, and used.
High performers understand that single numbers rarely tell the whole story. Calcium metabolism is a system – optimize the system, not just the number. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Calcium levels and mineral metabolism require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.