
The CO2 on your metabolic panel does not measure the carbon dioxide gas you exhale. It measures bicarbonate – the primary buffer in your blood that regulates acid-base balance and keeps your blood pH within the narrow range compatible with life. Your kidneys and lungs work together constantly to maintain this balance, and the CO2 (bicarbonate) level on your blood panel gives you a window into how well that regulatory system is functioning. An abnormal CO2 can reveal problems with your kidneys, lungs, metabolic health, acid production, and electrolyte status – making it a deceptively important marker that most people glance past without understanding what it is actually telling them.
What Is CO2 (Bicarbonate) on a Blood Panel?
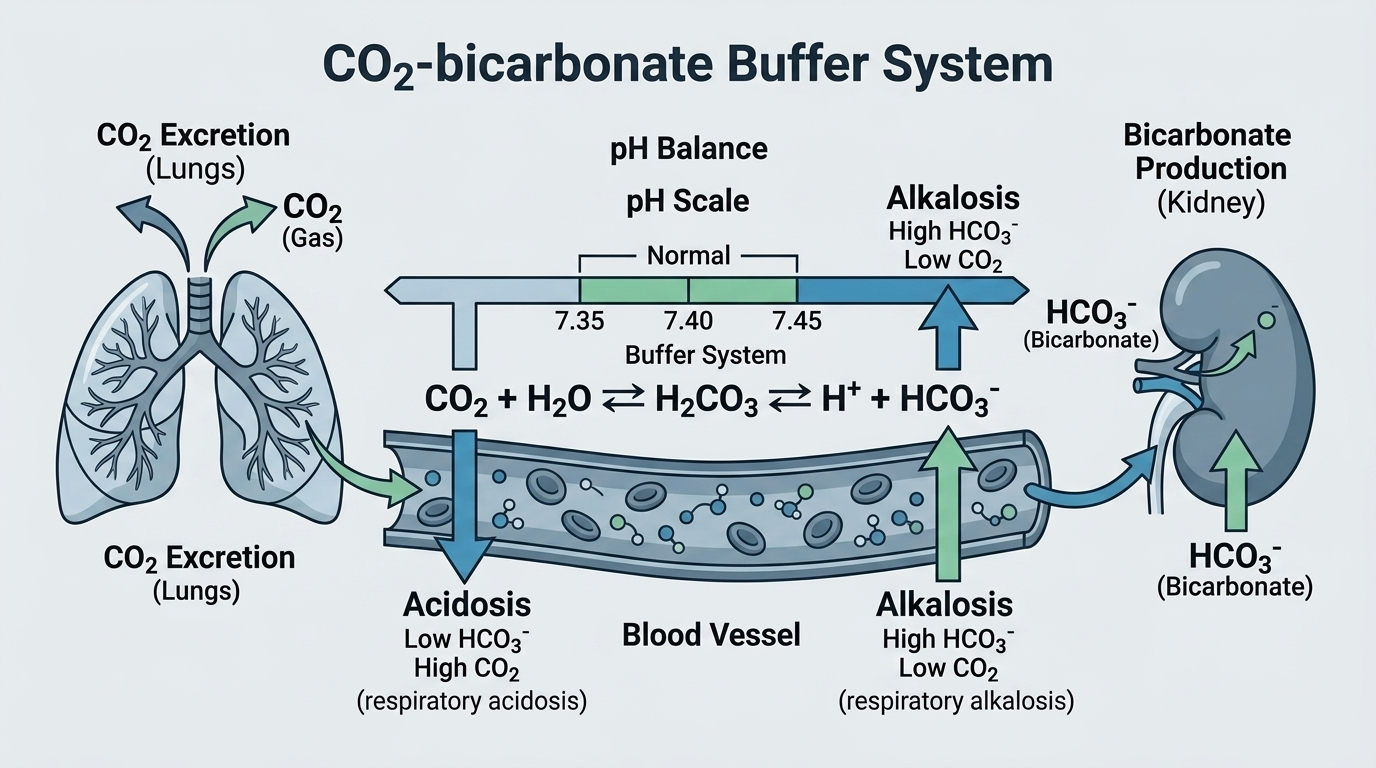
The CO2 reported on a basic or comprehensive metabolic panel is actually total carbon dioxide, which in practice approximates bicarbonate (HCO3-) – the main alkaline buffer in your blood. Bicarbonate is produced by the kidneys and represents the kidney’s primary mechanism for regulating blood pH. When the body produces excess acid (from metabolism, diet, or disease), the kidneys excrete acid and generate more bicarbonate to neutralize it. When the body is too alkaline, the kidneys excrete bicarbonate and retain acid. This system works in constant coordination with your lungs, which regulate CO2 gas levels in blood by adjusting breathing rate and depth.
The relationship is captured in the Henderson-Hasselbalch equation, but the practical insight is simpler: low bicarbonate (low CO2 on the panel) suggests metabolic acidosis – your body is either producing too much acid or losing too much bicarbonate. High bicarbonate suggests metabolic alkalosis – your body is either losing too much acid or retaining too much bicarbonate. Both states have performance implications, clinical significance, and underlying causes that deserve investigation rather than dismissal.
Why CO2/Bicarbonate Matters for Performance and Health
Blood pH is one of the most tightly regulated variables in human physiology. Even small deviations from the normal range (7.35-7.45) cause significant physiological dysfunction – enzymes stop working properly, oxygen delivery is impaired, cardiac function deteriorates. Your bicarbonate level is the primary indicator of how well your kidneys and metabolic systems are maintaining this critical balance. Chronic mild metabolic acidosis – bicarbonate trending toward the lower end of normal, often driven by high-protein diets, kidney function decline with age, or high dietary acid load – has been linked to accelerated muscle loss, bone density reduction, kidney stone formation, and insulin resistance. This is a subtle but important longevity concern that standard medicine rarely addresses until bicarbonate falls clearly below the reference range.
For athletes, bicarbonate is directly relevant to high-intensity performance. Intense exercise generates lactic acid, which temporarily lowers blood pH. Your buffering capacity – heavily dependent on bicarbonate – determines how long you can sustain high-intensity output before acidosis forces you to slow down. This is why bicarbonate loading (a practice used by some endurance and high-intensity athletes) has documented ergogenic effects on performance lasting 1-7 minutes of near-maximal effort. Understanding your resting bicarbonate and acid-base status is the foundation for understanding your buffering capacity.
Normal vs. Optimal CO2 Levels
Standard Reference Ranges: Most laboratories report CO2 (bicarbonate) as normal between 22 and 29 mEq/L (or mmol/L). Below 22 mEq/L suggests metabolic acidosis. Above 29 mEq/L suggests metabolic alkalosis. These boundaries have meaningful clinical validity – outside these ranges, the body’s acid-base regulatory systems are under significant stress.
The Problem With “Normal”: Bicarbonate at 23 mEq/L and 28 mEq/L are both “normal.” From a longevity and performance perspective, they are not equivalent. Research in chronic kidney disease populations shows that bicarbonate trending toward the lower end of normal (22-24 mEq/L) is associated with faster kidney function decline, greater muscle protein catabolism, and worse metabolic outcomes compared to bicarbonate in the 25-28 mEq/L range. People eating very high protein diets or very low carbohydrate diets often trend toward lower bicarbonate as the body handles the increased dietary acid load from protein metabolism.
Optimal CO2 for Longevity and Performance: For most adults, bicarbonate between 24 and 28 mEq/L represents the zone where acid-base regulation is efficient and the body is not under chronic acid-buffering stress. Consistently below 24 mEq/L warrants investigation of dietary acid load, early kidney function, and other causes of metabolic acidosis. Consistently above 28-29 mEq/L warrants investigation of potential metabolic alkalosis from diuretics, vomiting, or potassium/chloride depletion.
What Causes Low CO2 (Metabolic Acidosis)?
Chronic kidney disease is the most clinically significant cause of chronically low bicarbonate – impaired kidneys cannot adequately excrete acid or generate bicarbonate, leading to progressive metabolic acidosis that accelerates kidney decline and muscle loss. Diabetic ketoacidosis (DKA) and alcoholic ketoacidosis produce dramatic bicarbonate drops through ketone acid accumulation. Lactic acidosis from shock, liver failure, or some medications (metformin in kidney-impaired patients) causes metabolic acidosis. High-protein, low-carbohydrate diets (ketogenic diets, carnivore diets) increase dietary acid load and can push bicarbonate to the lower end of normal or below, particularly in people with any kidney function impairment. Diarrhea causes bicarbonate losses through the gut. Renal tubular acidosis (a group of kidney tubule disorders) impairs acid excretion. Certain toxins including methanol, ethylene glycol, and salicylate overdose cause severe metabolic acidosis. Respiratory alkalosis from hyperventilation causes compensatory bicarbonate lowering to maintain pH.
What Causes High CO2 (Metabolic Alkalosis)?
Vomiting or nasogastric suction causes massive loss of hydrochloric acid from the stomach, generating metabolic alkalosis with rising bicarbonate. Loop and thiazide diuretics cause metabolic alkalosis through potassium and chloride losses that trigger compensatory bicarbonate retention. Potassium depletion independently causes metabolic alkalosis through complex renal mechanisms. Excessive antacid or sodium bicarbonate use raises bicarbonate directly. Primary hyperaldosteronism (excess aldosterone) causes metabolic alkalosis through potassium wasting and hydrogen ion excretion. Chronic obstructive pulmonary disease (COPD) with chronic CO2 retention causes compensatory bicarbonate elevation as the kidneys retain bicarbonate to match the chronically elevated CO2. Bartter and Gitelman syndromes – rare inherited kidney disorders – cause metabolic alkalosis through tubular salt wasting.
CO2 and Kidney Health
The relationship between bicarbonate and kidney health is bidirectional and clinically critical. Low bicarbonate damages kidneys – chronic metabolic acidosis accelerates the progression of chronic kidney disease through multiple mechanisms including inflammation and fibrosis. Damaged kidneys lower bicarbonate – as kidney function declines, the ability to excrete acid and generate bicarbonate diminishes, creating a vicious cycle. Monitoring bicarbonate is therefore one of the most sensitive indicators of kidney stress that a basic metabolic panel provides. If bicarbonate is trending down over serial measurements – even within the “normal” range – it may indicate progressive kidney function decline worth investigating with more sensitive kidney function tests before eGFR falls dramatically.
Frequently Asked Questions
Is CO2 on a blood panel the same as CO2 in exhaled air?
No – they are related but different. The CO2 on a blood panel measures total carbon dioxide, which primarily reflects bicarbonate dissolved in the blood – the kidney-regulated acid-base buffer. Exhaled CO2 reflects CO2 gas being removed from blood by the lungs – the lung-regulated side of acid-base balance. The two systems work together (rising bicarbonate causes the lungs to retain more CO2 gas; falling bicarbonate causes the lungs to breathe off more CO2) but are distinct measurements of different things.
Can a low-carb diet affect my CO2 level?
Yes. High-protein and very low carbohydrate diets increase dietary acid load through sulfuric acid generated from protein metabolism and through ketone body production. This can push bicarbonate toward the lower end of normal (22-24 mEq/L). For most healthy people with normal kidney function, this is compensated normally. For people with any degree of kidney impairment, even modest dietary acid loading from high protein intake can accelerate bicarbonate decline. Increasing vegetable and fruit intake – which provides alkaline load – helps buffer the acid load from high protein intake.
What does low CO2 indicate on a routine blood panel?
Low CO2 (below 22 mEq/L) on a routine panel warrants investigation rather than dismissal. In the absence of obvious causes like acute illness, vomiting, or known diarrhea, persistently low bicarbonate suggests early kidney disease, a high dietary acid load, renal tubular acidosis, or occult metabolic acidosis from another cause. It should prompt kidney function testing (eGFR, creatinine, urine protein), medication review, and dietary assessment at minimum.
Does bicarbonate affect athletic performance?
Directly, yes. Bicarbonate is the primary blood buffer that neutralizes lactic acid produced during high-intensity exercise. Higher buffering capacity (supported by optimal bicarbonate) allows sustained higher-intensity effort before acidosis forces performance decline. Some athletes use sodium bicarbonate loading (typically 0.3 g/kg body weight) before competition as an ergogenic aid with evidence supporting improved performance in events lasting 1-7 minutes. Maintaining optimal resting bicarbonate through diet and kidney health is the foundation for buffering capacity.
Testing CO2 With ApexBlood
CO2 (bicarbonate) is included in ApexBlood’s comprehensive metabolic panel alongside kidney function markers, electrolytes, and metabolic indicators that provide the context needed to interpret your acid-base status accurately. Trending bicarbonate over time alongside eGFR and creatinine gives you an early warning system for kidney health changes before they become clinically severe.
You cannot optimize what you do not measure. Understanding your acid-base status and kidney health trend is foundational to long-term metabolic optimization.
Get comprehensive testing for $189
The Bottom Line on CO2 (Bicarbonate)
Bicarbonate is your blood’s primary acid-base buffer and your kidneys’ primary contribution to pH regulation. A normal CO2 means your regulatory system is maintaining the balance required for life. A trending-down CO2 – even within the normal range – can be an early signal of kidney stress, excessive dietary acid load, or metabolic dysfunction worth addressing before it becomes clinically significant. For high performers, optimal bicarbonate supports the buffering capacity that enables sustained high-intensity effort and rapid recovery from metabolic acidosis during training.
Understand your acid-base status. Do not dismiss a low-normal CO2 as “fine.” And do not wait for a clearly abnormal value before investigating the trend. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Bicarbonate levels and acid-base status require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.