
Chloride is the most abundant anion (negatively charged ion) in your blood and extracellular fluid. It works in close partnership with sodium to maintain fluid balance, blood volume, and the electrical neutrality of your blood. Chloride does not get the attention that sodium and potassium receive, partly because isolated chloride abnormalities are unusual – chloride typically moves in sync with sodium and in inverse relationship with bicarbonate. But chloride is a critical piece of the acid-base puzzle, and understanding what your chloride level means in the context of your other electrolytes reveals important information about your metabolic state, kidney function, and respiratory efficiency that no single marker can tell you alone.
What Is Serum Chloride?
Chloride is the negatively charged counterpart to sodium in your extracellular fluid. Where sodium goes, chloride typically follows to maintain electrical neutrality in blood. Chloride is absorbed from food in the gut, filtered and reabsorbed by the kidneys, and excreted in urine at a rate regulated by the same mechanisms that control sodium. The chloride content of body fluids is highest in gastric acid (hydrochloric acid), which is why vomiting causes dramatic chloride losses. Chloride also plays a direct role in acid-base balance – as bicarbonate (the primary blood buffer) rises, chloride falls proportionally to maintain electrical neutrality, and vice versa. This inverse relationship between chloride and bicarbonate is the key to using chloride as an acid-base diagnostic tool.
Why Chloride Matters
Chloride’s clinical value is largely as an indicator of fluid-electrolyte balance and acid-base status. On its own, chloride tells you relatively little. In context with sodium, bicarbonate (CO2), potassium, and anion gap, chloride becomes a powerful tool for identifying metabolic alkalosis, metabolic acidosis, respiratory compensation states, and dehydration patterns. For high performers, the most practically relevant chloride insight is what it reveals about hydration status and the body’s acid-base regulation during high-intensity training, prolonged endurance activity, and dietary interventions like very low carbohydrate eating that shift acid-base balance.
Normal vs. Optimal Chloride Levels
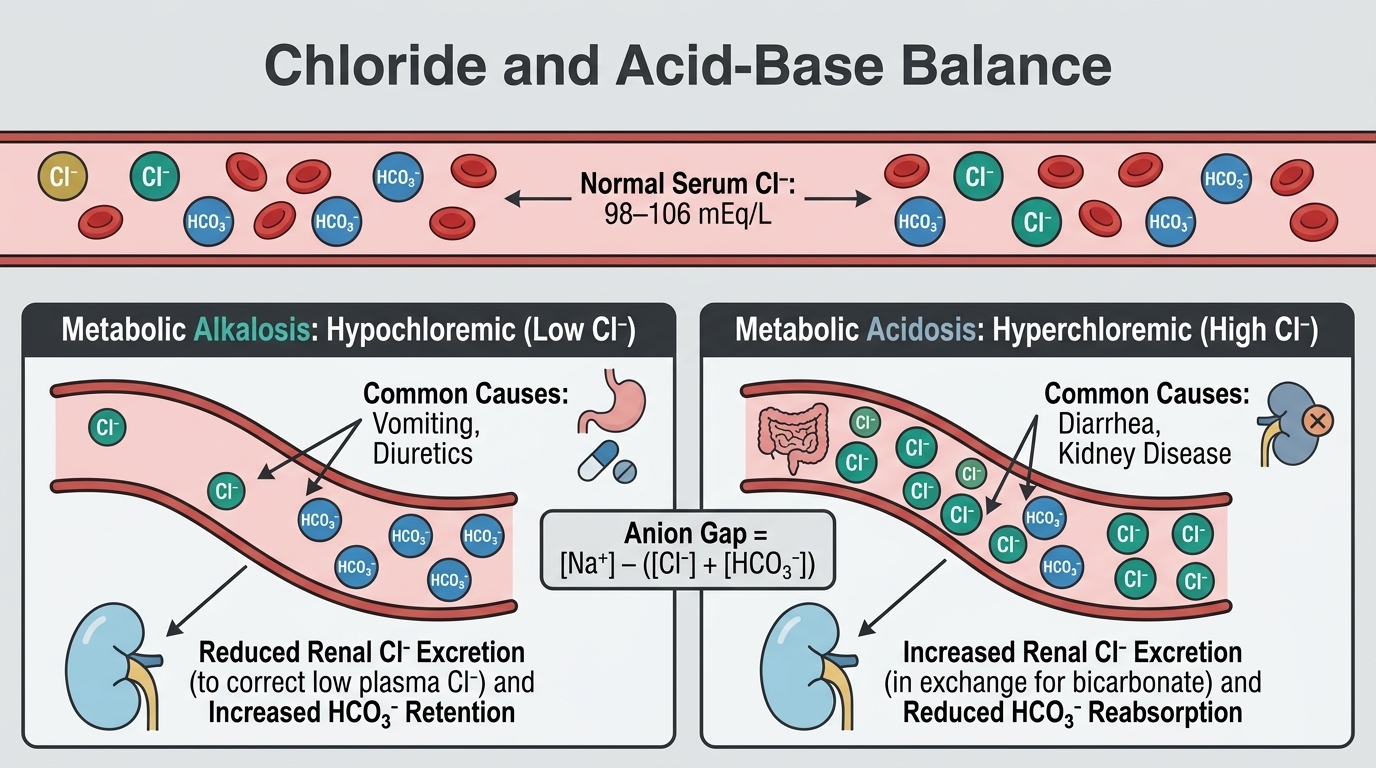
Standard Reference Ranges: Most laboratories report serum chloride as normal between 98 and 106 mEq/L (or mmol/L). These ranges are derived from population studies and reflect the narrow physiological regulation of chloride in concert with sodium and bicarbonate. Unlike some reference ranges that are excessively broad, the chloride reference range is reasonably clinically useful.
Optimal Chloride Within the Range: For most healthy adults, chloride in the middle of the reference range (100-104 mEq/L) alongside normal sodium and bicarbonate suggests well-regulated electrolyte and acid-base status. Chloride at the lower end of normal (98-100 mEq/L) alongside high bicarbonate suggests metabolic alkalosis – a state often seen after vomiting, with diuretic use, or in states of potassium depletion. Chloride at the upper end of normal or above normal (above 106 mEq/L) alongside low bicarbonate suggests hyperchloremic metabolic acidosis – seen in early kidney disease, diarrhea, renal tubular acidosis, or after certain intravenous fluid administration. Neither extreme is trivial to dismiss.
What Causes Low Chloride (Hypochloremia)?
Vomiting is the classic and most dramatic cause of hypochloremia – gastric acid (hydrochloric acid) contains high concentrations of chloride, and significant vomiting depletes chloride rapidly while generating metabolic alkalosis. Nasogastric suctioning in hospitalized patients causes the same effect. Loop and thiazide diuretics increase urinary chloride excretion alongside sodium, causing hypochloremia. Metabolic alkalosis from any cause (excessive antacid use, hypokalemia, severe potassium depletion) is accompanied by low chloride. Profuse sweating during extreme endurance exercise causes chloride losses alongside sodium. Excessive water intake without electrolyte replacement (dilution effect) can lower chloride along with sodium. Adrenal insufficiency and certain kidney disorders can impair chloride handling.
What Causes High Chloride (Hyperchloremia)?
Dehydration is the most common cause – as water is lost without proportional electrolyte loss, chloride concentration rises. Diarrhea causes disproportionate bicarbonate losses relative to chloride, resulting in hyperchloremic metabolic acidosis. Renal tubular acidosis – a group of kidney disorders impairing acid excretion – causes hyperchloremia through bicarbonate wasting. Excessive normal saline administration (which contains 154 mEq/L of chloride, higher than blood) causes hyperchloremic acidosis. High dietary sodium chloride intake relative to water intake can mildly elevate chloride. Respiratory alkalosis (hyperventilation causing excess CO2 loss) produces compensatory chloride retention to maintain charge balance. Early chronic kidney disease often shows hyperchloremia before other kidney function markers become abnormal.
Chloride and Anion Gap
One of chloride’s most important clinical applications is in calculating the anion gap – a calculated value that helps identify the cause of metabolic acidosis. The anion gap is calculated as: Sodium – (Chloride + Bicarbonate). The normal anion gap is approximately 8-12 mEq/L. High anion gap metabolic acidosis (where unmeasured anions are accumulating – from ketones in diabetic ketoacidosis, lactate in shock, or toxins like methanol) is distinguished from normal anion gap (hyperchloremic) metabolic acidosis by this calculation. In normal anion gap acidosis, chloride is elevated because as bicarbonate is lost, chloride rises to maintain electroneutrality. This distinction completely changes the clinical approach and treatment. Chloride is essential to making this critical diagnostic distinction.
Frequently Asked Questions
Is chloride the same as salt?
Not exactly, but they are closely related. Table salt is sodium chloride (NaCl) – one sodium ion paired with one chloride ion. When salt dissolves in the body, it separates into sodium and chloride ions. Dietary chloride intake is therefore largely determined by sodium intake from salt. A high-sodium diet is also a high-chloride diet. This is one reason why chloride tracks so closely with sodium on blood panels.
Can low chloride cause symptoms?
Mild hypochloremia often produces no specific symptoms because it typically occurs alongside hyponatremia (which causes the dominant symptoms) or metabolic alkalosis (which causes muscle twitching, weakness, and cognitive changes). Severe isolated hypochloremia is rare. Most chloride-related symptoms are actually symptoms of the accompanying electrolyte imbalance or acid-base disturbance rather than the chloride abnormality itself.
What does a high chloride with low bicarbonate mean?
High chloride alongside low bicarbonate is the hallmark of hyperchloremic (normal anion gap) metabolic acidosis. This pattern should prompt investigation of causes including diarrhea with bicarbonate loss, renal tubular acidosis, early kidney disease, the use of carbonic anhydrase inhibitors (like acetazolamide), or excessive normal saline infusion in hospitalized patients. It is not a pattern to dismiss as a benign laboratory variation.
How does chloride relate to blood pressure?
Some research suggests that chloride itself – not just sodium – contributes to blood pressure elevation in salt-sensitive individuals. Studies using sodium bicarbonate versus sodium chloride suggest that the chloride component of dietary salt may independently raise blood pressure beyond the sodium effect alone. This is a nuanced area of ongoing research, but it supports the general principle that reducing processed food intake (which is heavily seasoned with sodium chloride) is likely beneficial for blood pressure independent of the sodium reduction alone.
Testing Chloride With ApexBlood
Chloride is reported as part of ApexBlood’s comprehensive metabolic panel alongside sodium, potassium, bicarbonate (CO2), BUN, creatinine, and glucose – the full basic metabolic panel that allows proper interpretation of acid-base status and electrolyte balance. Chloride in isolation is a limited test. In context with the full panel, it becomes a valuable diagnostic tool for identifying fluid imbalances, acid-base abnormalities, and early kidney dysfunction.
Get comprehensive testing for $189
The Bottom Line on Chloride
Chloride is the unsung electrolyte that ties your fluid balance and acid-base regulation together. Most people and most physicians give it little independent attention – and that is often appropriate, because isolated chloride abnormalities are uncommon. But chloride in context with bicarbonate and sodium is one of the most diagnostically powerful components of a basic metabolic panel, pointing toward acid-base disturbances that have major implications for kidney health, hydration status, and metabolic function. Understanding your complete electrolyte picture means understanding chloride’s role in the system. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Chloride and electrolyte status require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.