
Creatinine is one of the most relied-upon kidney function markers in clinical medicine, yet it has significant blind spots that make it an imperfect screening tool when used in isolation. Creatinine is a waste product of creatine phosphate metabolism in muscle tissue – produced at a relatively constant rate proportional to muscle mass and excreted by the kidneys. When kidney filtration capacity falls significantly, creatinine accumulates in the blood. But creatinine only rises meaningfully after substantial kidney function has already been lost – and in individuals with very low muscle mass, creatinine can appear falsely reassuring even when filtration is compromised. Understanding what creatinine actually tells you – and where it falls short – is essential for anyone serious about long-term kidney health and metabolic optimization.
What Is Creatinine?
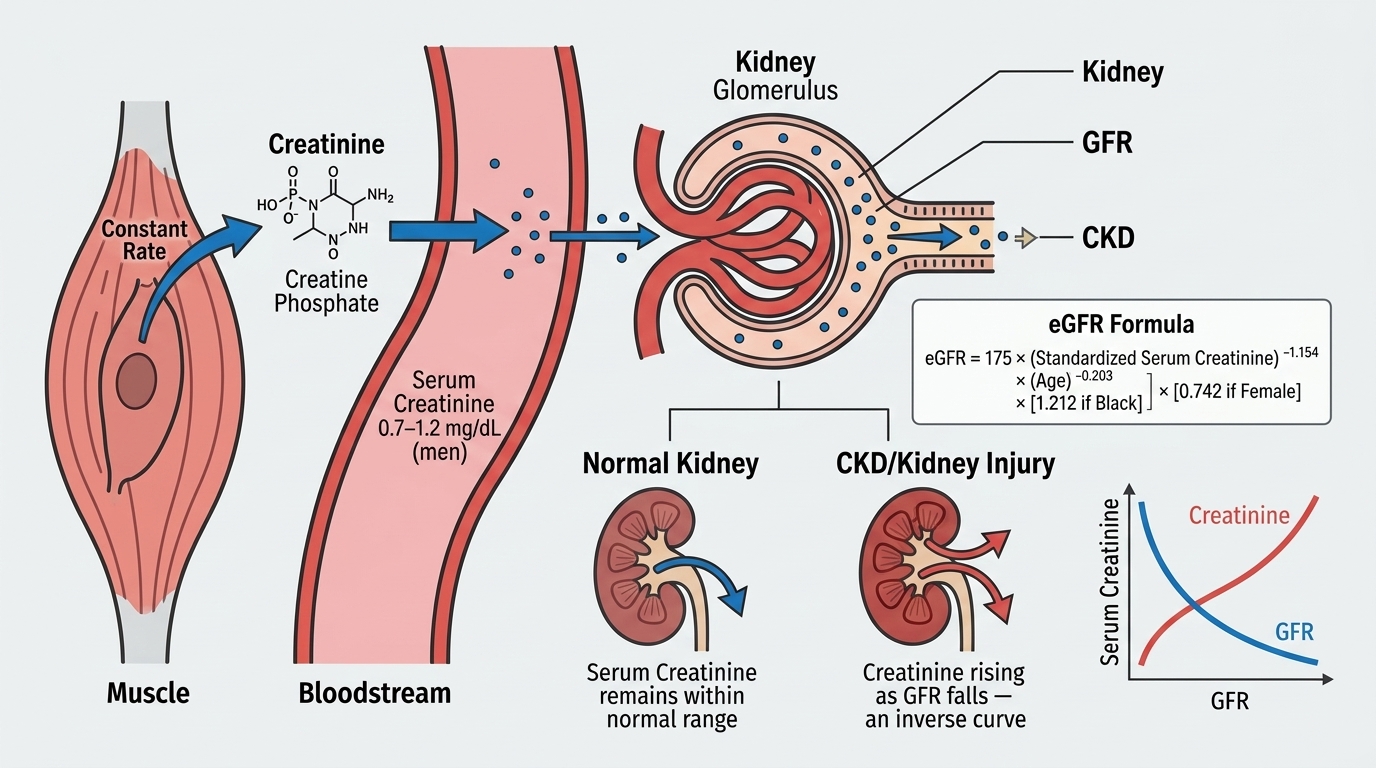
Creatinine is a byproduct of creatine phosphate breakdown in skeletal muscle. Creatine phosphate is the rapid energy reserve that replenishes ATP during high-intensity muscle contractions – the same compound that many athletes supplement in the form of creatine monohydrate. As creatine phosphate is used and regenerated, a small percentage is irreversibly converted to creatinine. This production occurs at a rate that is proportional to total skeletal muscle mass and is remarkably consistent day-to-day in healthy individuals, making creatinine a useful steady-state marker of kidney filtration efficiency.
The kidneys filter creatinine from the blood through the glomeruli and excrete it in urine with minimal reabsorption. When glomerular filtration rate (GFR) declines, creatinine clears more slowly and accumulates in the bloodstream. This is why serum creatinine is used to estimate GFR – the calculation that produces the eGFR value on your metabolic panel. The eGFR incorporates creatinine, age, and sex (and optionally race) to estimate how much blood the kidneys are filtering per minute, expressed as mL/min/1.73m².
Why Creatinine Matters for Performance and Longevity
Kidney function is one of the most important determinants of long-term health outcomes. Chronic kidney disease (CKD) affects an estimated 37 million Americans and is strongly associated with accelerated cardiovascular disease, hypertension, anemia, bone disease, and reduced lifespan. The critical problem with CKD is that it is completely asymptomatic until function has declined substantially – often 50% or more of kidney capacity can be lost before any symptoms appear. Creatinine and eGFR monitoring is one of the primary methods for detecting this decline early, when interventions are most effective.
For health optimizers and performance-focused individuals, creatinine also matters in the context of muscle mass and training adaptations. Athletes and people with high muscle mass will naturally have higher baseline creatinine than sedentary individuals with low muscle mass – not from kidney disease but from the higher total creatine pool generating more creatinine. Creatine supplementation, high meat intake, and intense exercise (especially eccentric or high-volume training) can transiently elevate creatinine. Understanding your baseline and how it responds to changes in training, diet, and hydration prevents unnecessary alarm and allows meaningful tracking of kidney function over time.
Normal vs. Optimal Creatinine Levels
Standard Reference Ranges: Laboratory reference ranges for serum creatinine are typically 0.74-1.35 mg/dL for adult males and 0.59-1.04 mg/dL for adult females. These ranges are wider than they appear to be because creatinine production is muscle-mass dependent, and there is substantial variation in muscle mass across the healthy adult population. A creatinine of 1.3 mg/dL might reflect excellent kidney function in a 220-pound muscular male and early kidney disease in a 110-pound sedentary female.
The Problem With “Normal”: A major limitation of creatinine as a standalone kidney function marker is that it is an insensitive test – serum creatinine only rises above the normal range after approximately 50-60% of kidney filtration capacity has already been lost. This is the “creatinine blind spot” – substantial kidney disease can exist with completely normal serum creatinine. This is why eGFR, calculated from creatinine, is preferred over creatinine alone: it provides a more sensitive estimate of filtration capacity across different body sizes and ages. eGFR above 90 mL/min/1.73m² is considered normal. eGFR 60-89 indicates mild reduction. eGFR 30-59 indicates moderate reduction. eGFR 15-29 indicates severe reduction. eGFR below 15 indicates kidney failure.
Optimal Creatinine for Your Body Type: Rather than a single number, optimal creatinine is interpreted in the context of your muscle mass and eGFR. A well-muscled adult male with creatinine of 1.1-1.3 mg/dL and eGFR above 90 has excellent kidney function. A petite adult female with creatinine of 0.7-0.9 mg/dL and eGFR above 90 similarly has excellent function. The trend over time matters as much as any single value – a creatinine that is rising progressively over years, even within the normal range, may signal declining kidney function worth investigating.
What Causes High Creatinine?
Acute kidney injury (AKI) from dehydration, medications, infections, toxins, or reduced blood flow to the kidneys causes creatinine to rise acutely over hours to days – this is a medical urgency that requires rapid evaluation. Chronic kidney disease from diabetes, hypertension, autoimmune conditions, or genetic disorders causes creatinine to rise gradually over months to years. Dehydration (without AKI) mildly elevates creatinine by reducing urinary flow and concentrating blood. High meat intake and creatine supplementation increase creatinine production. Large muscle mass elevates baseline creatinine. Intense resistance training or endurance exercise can cause transient creatinine elevation from muscle breakdown and increased creatinine production. Certain medications – including some antibiotics (trimethoprim, cimetidine) and NSAID pain relievers – elevate creatinine through mechanisms that do not reflect true GFR decline.
What Causes Low Creatinine?
Low muscle mass – from aging (sarcopenia), malnutrition, prolonged immobility, or neuromuscular disease – reduces creatinine production and lowers serum creatinine. This is why very low creatinine can be a marker of poor nutritional status or inadequate muscle mass rather than exceptional kidney function. Pregnancy causes hemodilution and increased renal blood flow, lowering creatinine. Advanced liver disease reduces muscle mass and creatinine production. Very low-protein diets (vegan diets without adequate protein, restrictive eating patterns) reduce creatinine production. In elderly individuals especially, low creatinine alongside low muscle mass can create a false impression of normal kidney function when eGFR is actually reduced.
Creatinine in the Context of Kidney Disease Prevention
The most impactful use of creatinine monitoring is as part of a longitudinal kidney health strategy. Tracking creatinine and eGFR annually (or more frequently with risk factors for CKD) allows detection of the gradual upward trend in creatinine and downward trend in eGFR that characterizes progressive kidney disease. The risk factors for CKD that make close monitoring especially important include: Type 2 diabetes (the leading cause of CKD), hypertension (the second leading cause), obesity, metabolic syndrome, family history of kidney disease, cardiovascular disease, and use of nephrotoxic medications (NSAIDs, certain antibiotics, contrast agents, some supplements).
Early CKD intervention – blood pressure control, blood sugar optimization, dietary modifications, nephrotoxin avoidance, and when appropriate disease-modifying medications – can dramatically slow or halt CKD progression. The window for intervention is much wider when decline is caught early at eGFR 75-90 versus late at eGFR 30-45. This is why annual monitoring matters even in people who feel completely healthy.
Frequently Asked Questions
Does creatine supplementation damage kidneys?
In individuals with healthy kidneys, creatine supplementation does not cause kidney damage. Creatine does increase serum creatinine because more creatine is being converted to creatinine, which can make it appear that kidney function has worsened when it has not. If you are on creatine supplementation and your creatinine is elevated but your eGFR is normal and stable, there is no evidence of kidney harm. The concern about creatine and kidneys is largely unfounded in healthy people, though individuals with pre-existing kidney disease should use caution and consult their physician before supplementing.
Why does my creatinine go up after hard workouts?
Intense exercise, particularly eccentric exercise like downhill running or heavy resistance training, causes temporary muscle breakdown (exercise-induced rhabdomyolysis in milder forms). This releases creatine kinase, myoglobin, and creatinine from muscle cells into the bloodstream. Creatinine can temporarily rise 0.1-0.3 mg/dL after hard training. Testing within 24-48 hours of intense exercise can produce a mildly elevated creatinine that normalizes after rest. For the most accurate kidney function assessment, blood draws are ideally done after 48-72 hours of rest from intense training.
What is eGFR and why does it matter more than creatinine alone?
eGFR (estimated glomerular filtration rate) is a calculated estimate of how much blood your kidneys are filtering per minute, adjusted for body surface area. It accounts for the fact that the same creatinine level means very different things in a 25-year-old 200-pound male versus a 75-year-old 130-pound female. eGFR makes kidney function comparable across age groups, sexes, and body sizes. It is a better indicator of true kidney filtration capacity than serum creatinine alone, though it is still an estimate and is most accurate when kidney function is stable (it is less reliable in acute kidney injury or extreme muscle mass).
At what creatinine level should I be concerned?
Rather than a single threshold, concerning patterns include: creatinine rising above your established baseline on multiple measurements, creatinine rising progressively over months to years even if still within the normal range, creatinine above the upper limit of normal for your sex, or eGFR below 60 on two or more measurements separated by at least three months. A single elevated creatinine often needs to be repeated along with BUN, electrolytes, and a urinalysis before drawing conclusions. Any creatinine that is doubled from baseline or accompanied by symptoms warrants urgent medical evaluation.
Can kidneys recover from an elevated creatinine?
It depends entirely on the cause. Acute kidney injury from dehydration, medications, or temporary reduced blood flow often improves or fully resolves with treatment – creatinine returns to baseline. Acute kidney injury from severe causes (sepsis, major surgery, toxins) can result in incomplete recovery and permanent GFR reduction. Chronic kidney disease from diabetes, hypertension, or structural damage does not typically reverse, but progression can be significantly slowed or halted with appropriate management. This distinction – acute versus chronic, reversible versus irreversible – is why evaluation of elevated creatinine requires clinical context, not just the number.
Testing Creatinine With ApexBlood
ApexBlood’s comprehensive panel includes creatinine, BUN, eGFR, electrolytes, and a full metabolic panel that allows complete kidney health assessment in context. You get the numbers and the interpretation – understanding what your creatinine means given your muscle mass, age, training habits, and metabolic profile. Our physicians are available to discuss any abnormalities and guide next steps for kidney health optimization.
Get comprehensive testing for $189
The Bottom Line on Creatinine
Creatinine is a valuable kidney function marker with important limitations – it is muscle-mass dependent, rises only after significant kidney function is already lost, and is affected by diet, exercise, supplementation, and hydration. Used alongside eGFR, BUN, and urine albumin, it becomes part of a comprehensive kidney health picture that can identify declining function years before symptoms develop. The goal is not just a “normal” creatinine – it is stable or improving kidney function that supports longevity, metabolic health, and performance across decades. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Creatinine and kidney function require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.