
Ferritin: The Iron Storage Marker That Predicts Performance Before Problems Appear
You’ve had your blood work done. The iron panel shows serum iron is normal. Hemoglobin is normal. Your doctor sees no red flags and moves on.
But your ferritin is 22 ng/mL.
That number – technically above the clinical deficiency threshold on most lab reports – is quietly explaining why you’re exhausted by 2pm, why your workouts feel harder than they should, why your hair is thinning despite adequate protein, why your brain isn’t operating at the sharpness you expect from yourself. You’re not anemic. You won’t get flagged. But your iron stores are depleted to the point where your biology is rationing resources, pulling from reserves that should be robust, and your performance is paying the price.
Ferritin is the single most important iron marker in routine blood testing – and the one most systematically misinterpreted by standard medicine. The reference range floor of 12-15 ng/mL on most lab reports represents the threshold below which clinical disease is diagnosed. It has nothing to do with optimal function. The gap between “not deficient” and “optimized” spans an enormous range of performance, energy, cognitive function, and physical capacity – and most people living in that gap have no idea it exists.
High performers don’t optimize to the floor of a reference range. They understand where their markers need to be for peak function and they test comprehensively enough to know where they actually stand.
What Is Ferritin?
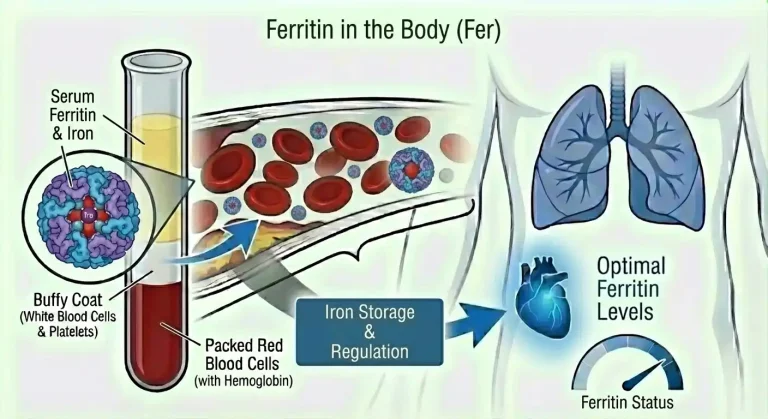
Ferritin is a protein whose primary function is iron storage. It acts as the body’s iron bank – capturing excess iron when it’s abundant, holding it safely in reserve, and releasing it when the body’s demand for functional iron exceeds what’s immediately available from diet and transport.
Structurally, ferritin is a hollow spherical protein shell composed of 24 subunits arranged around a central cavity that can store up to 4,500 iron atoms in a stable, non-toxic form. This structure is critical because free iron – iron not bound to a protein – is chemically reactive and dangerous. Free iron catalyzes the production of free radicals through a reaction called Fenton chemistry, generating hydroxyl radicals that damage DNA, proteins, and cell membranes. Ferritin neutralizes this reactivity by sequestering iron in a controlled, accessible storage form.
Ferritin is distributed throughout the body with the highest concentrations in the liver (the primary iron storage organ), spleen, and bone marrow – the sites most involved in red blood cell production and recycling. Skeletal muscle contains myoferritin, and virtually every cell in the body expresses some ferritin because iron management is a universal cellular requirement.
A small amount of ferritin continuously leaks from cells into the bloodstream. This circulating serum ferritin doesn’t perform the same storage function as intracellular ferritin, but its concentration in blood closely reflects the total body iron store – making serum ferritin the most practical and reliable indirect measure of iron storage status available through routine blood testing.
The relationship between serum ferritin and total body iron stores is approximately linear across the normal range: each 1 ng/mL of serum ferritin corresponds to roughly 8-10 mg of stored body iron. A person with ferritin at 15 ng/mL has approximately 120-150 mg of stored iron – barely enough to maintain hemoglobin production if dietary iron is interrupted for even a short period. A person with ferritin at 100 ng/mL has approximately 800-1,000 mg of stored iron – robust reserves that buffer against dietary inadequacy, increased demand, and acute blood loss without immediate functional consequences.
This reserve capacity is the entire point of iron storage. Ferritin exists so that your body has a buffer between iron intake and iron need – a buffer that allows you to navigate variation in dietary intake, illness-related appetite suppression, increased iron demand from training or growth, and minor blood losses without immediately compromising the iron-dependent processes that determine how you feel and perform.
When that buffer is depleted, you lose resilience. Every stressor becomes a potential trigger for functional decline.
Why Ferritin Matters for Performance and Health
Ferritin’s significance extends well beyond being a simple storage depot. It’s the leading indicator of iron status – the earliest marker to shift as iron stores deplete, long before serum iron, transferrin saturation, or hemoglobin show abnormalities. For performance-focused individuals, this predictive quality is exactly what makes ferritin the most actionable iron marker available.
Ferritin falls first in iron depletion. The sequence of iron deficiency development is well characterized: ferritin drops as stores are depleted, while serum iron, transferrin saturation, and hemoglobin remain normal. This stage – called iron depletion or pre-latent iron deficiency – can persist for months or years before progressing to the stages where other markers become abnormal. People in this stage feel the functional consequences of depleted iron stores while receiving completely normal results on the markers most physicians actually review. Ferritin is the only standard marker that catches iron deficiency at this earliest, most reversible stage.
Low ferritin causes symptoms independent of anemia. This is the most clinically underappreciated fact about ferritin. Research consistently demonstrates that fatigue, impaired exercise capacity, reduced cognitive function, and hair loss appear at ferritin levels well above the anemia threshold – typically below 30-50 ng/mL – in individuals whose hemoglobin remains entirely normal. A landmark study in women with unexplained fatigue and ferritin below 50 ng/mL but normal hemoglobin found that iron supplementation producing ferritin repletion significantly reduced fatigue independent of any change in hemoglobin. The mechanism is direct cellular iron dependency – tissues require iron for mitochondrial function, neurotransmitter synthesis, and enzyme activity independent of hemoglobin’s oxygen transport role.
Athletic performance is acutely sensitive to ferritin status. Sports medicine and exercise science research has established clear ferritin thresholds below which performance is measurably impaired. Most sports medicine practitioners use ferritin targets of 50-75 ng/mL as the minimum for recreational athletes, 75-100 ng/mL for competitive athletes, and some endurance specialists target 100-150 ng/mL for elite performers. Athletes with ferritin in the 20-40 ng/mL range – technically above the clinical deficiency floor – consistently show reduced VO2 max, earlier lactate threshold, greater perceived exertion at submaximal workloads, and slower post-exercise recovery compared to athletes with ferritin above 75-100 ng/mL.
Cognitive function tracks ferritin status closely. The brain has high iron demands for neurotransmitter synthesis – dopamine, serotonin, and norepinephrine all require iron-dependent enzymes for their production. Ferritin depletion impairs these pathways before anemia develops, producing the cognitive symptoms that ferritin-deficient individuals often describe as their most disabling: difficulty concentrating, reduced working memory, slowed information processing, decision fatigue, and motivational flatness. These cognitive effects are dose-dependent – they appear earlier and more severely at lower ferritin levels and improve progressively as ferritin is repleted.
Hair follicle function depends on adequate iron stores. Hair follicles are among the most metabolically active tissues in the body – they have high iron requirements for the rapid cell division that produces hair fiber. When iron stores are depleted, the body prioritizes iron delivery to critical systems (oxygen transport, brain function) at the expense of non-essential tissues including hair follicles. This triggers telogen effluvium – a form of diffuse hair shedding where follicles prematurely enter the resting phase and shed. Low ferritin is one of the most common and most overlooked reversible causes of hair loss, and ferritin repletion – targeting levels above 70-100 ng/mL – consistently improves hair retention in ferritin-deficient individuals.
Thyroid function is supported by adequate iron stores. Thyroid peroxidase – the enzyme that synthesizes thyroid hormones T3 and T4 – is iron-dependent. Depleted ferritin impairs thyroid hormone synthesis and reduces T4-to-T3 conversion, contributing to functional hypothyroid symptoms – fatigue, cold intolerance, slowed metabolism, weight management difficulty, and cognitive fog – even when TSH and thyroid hormone levels appear technically normal. People experiencing these symptoms should have ferritin assessed alongside thyroid markers, because iron repletion alone sometimes resolves apparent thyroid symptoms without any thyroid-specific intervention.
Immune resilience requires robust iron stores. Immune cells – particularly lymphocytes and macrophages – have high iron demands during immune activation. Depleted ferritin compromises immune cell proliferation and function, slowing the response to infections and prolonging recovery time. People who find themselves getting sick frequently or recovering from illness more slowly than expected should have ferritin on their assessment list.
Restless legs syndrome (RLS) is strongly associated with low ferritin, with a well-established clinical recommendation to replete ferritin above 50-75 ng/mL in affected individuals. Iron is required for dopamine synthesis in the substantia nigra – the brain region whose dysfunction underlies RLS – and brain iron status correlates with serum ferritin. Many people with RLS find that ferritin optimization significantly reduces symptoms without pharmaceutical intervention.
Normal vs. Optimal Ferritin Levels
This is where the gap between standard medicine and performance optimization is most stark and most consequential.
Standard laboratory reference ranges:
Women: 12-150 ng/mL (some labs use 11-307 ng/mL) Men: 30-400 ng/mL (some labs use 24-336 ng/mL)
These ranges are population-derived statistical intervals – they capture the middle 95% of values in a reference population that includes sedentary individuals, people with suboptimal nutrition, and varying degrees of chronic illness. The lower bounds represent the threshold below which clinical iron deficiency anemia is likely imminent – not the threshold below which function is impaired.
The problem with “normal”: A woman with ferritin at 14 ng/mL is technically within the reference range on many lab reports. She may receive no flag, no comment, and no intervention. She also has iron stores so depleted that a modest increase in demand – a period of heavy training, a viral illness, a few heavy menstrual cycles – could push her into frank anemia. In the meantime, she’s likely experiencing symptoms of functional iron deficiency that are being attributed to stress, aging, or other causes.
The clinical distinction medicine draws is between iron deficiency anemia (below the reference range floor) and normal (above it). The distinction that matters for performance is between depleted stores and replete stores – a distinction that requires a much higher ferritin threshold.
Optimal ferritin for performance and health:
General optimal range: 70-150 ng/mL (men and women) Minimum for symptomatic individuals: 50 ng/mL Target for active individuals: 100-150 ng/mL Target for endurance athletes: 100-175 ng/mL
The evidence supporting these targets comes from multiple domains – studies on non-anemic iron deficiency and cognitive function, sports medicine research on athletic performance and ferritin thresholds, dermatology research on hair loss and ferritin, and clinical experience with functional iron deficiency treatment. Collectively, they point to ferritin well above 50 ng/mL as the minimum for individuals pursuing optimal function, with 100+ ng/mL providing more robust reserves.
The upper end matters too. Ferritin above 200-300 ng/mL in the absence of known inflammatory conditions should prompt investigation. In men and postmenopausal women particularly, progressively rising ferritin can indicate hereditary hemochromatosis – a common genetic condition causing progressive iron overload with serious organ consequences. Very high ferritin (above 500-1,000 ng/mL) warrants thorough evaluation for iron overload disorders, significant liver disease, or systemic inflammatory conditions regardless of sex or age.
What Causes Low Ferritin?
Ferritin depletes whenever iron losses or demands exceed iron intake and absorption over time. The specific drivers determine both the rate of depletion and the appropriate intervention.
Inadequate dietary iron intake is the foundational cause in many people. Plant-based and vegan diets eliminate heme iron – the most bioavailable dietary iron form – relying entirely on non-heme iron with its inherently lower and more variable absorption. Even well-planned plant-based diets require substantially higher dietary iron targets to achieve the same stored iron as diets containing moderate amounts of red meat and other heme iron sources. People following calorie-restricted diets for weight management often simultaneously restrict iron intake below adequate levels without realizing it.
Menstruation is the most common cause of chronically low ferritin in otherwise healthy premenopausal women. Monthly blood loss of 30-80 mL – or significantly more in women with heavy periods – creates a recurring iron deficit that compounds over years without deliberate dietary emphasis on iron intake or supplementation. Many women with lifelong ferritin in the 15-40 ng/mL range have simply never compensated for the cumulative iron losses of their menstrual cycles. Heavy menstrual bleeding (more than 80 mL per cycle) makes ferritin maintenance through diet alone nearly impossible for most women and virtually requires supplementation.
Intense and high-volume training depletes ferritin through multiple mechanisms simultaneously. Foot-strike hemolysis in running athletes destroys red blood cells mechanically, releasing hemoglobin that is cleared renally and represents direct iron loss. High training volumes dramatically increase red blood cell turnover and erythropoiesis, consuming iron stores at rates that can exceed dietary supply. Exercise-induced inflammatory responses elevate hepcidin transiently, reducing iron absorption in the hours following intense training sessions. Sweat losses, while minor per session, accumulate meaningfully over high training volumes. The combination produces iron drain rates that frequently exceed what athletes consume – making ferritin monitoring a standard of care in serious athletic training.
Gastrointestinal blood loss is the most important cause of ferritin depletion to identify promptly, because it may signal significant pathology. Chronic low-level bleeding from peptic ulcers, gastritis, esophagitis, hemorrhoids, arteriovenous malformations, inflammatory bowel disease, polyps, or colorectal cancer depletes iron stores progressively without producing obvious symptoms until anemia is advanced. Any man or postmenopausal woman with unexplained low ferritin should have gastrointestinal evaluation before assuming dietary insufficiency. In premenopausal women, GI evaluation should be pursued when ferritin remains low despite adequate dietary iron and supplementation, or when the degree of depletion is disproportionate to menstrual loss alone.
Impaired iron absorption prevents stores from being replenished even with adequate dietary intake. Celiac disease is the most impactful – the villous damage of untreated celiac dramatically reduces iron absorption surface area, producing profound ferritin depletion that responds to gluten elimination rather than iron supplementation alone. H. pylori infection reduces gastric acid and impairs the conversion of dietary iron to its absorbable form – ferritin often normalizes after H. pylori eradication without any change in diet or supplementation. Proton pump inhibitor use chronically reduces gastric acid with similar effects on iron absorption over time. Inflammatory bowel disease affects both absorption surface area and creates ongoing blood loss.
Frequent blood donation depletes ferritin progressively in regular donors. Each unit of donated whole blood contains approximately 200-250 mg of iron – a substantial fraction of total body iron stores. Donors giving 3-4 or more times per year commonly develop progressively lower ferritin even without other contributing factors. Blood donation organizations generally recommend iron supplementation for regular donors and minimum ferritin thresholds before donation to protect donors – but follow-through monitoring is inconsistent.
Pregnancy creates enormous iron demands as maternal blood volume expands and fetal iron requirements must be met entirely from maternal stores. Ferritin commonly falls substantially across pregnancy even with iron supplementation – postpartum ferritin depletion is extremely common and frequently unaddressed, contributing to postpartum fatigue that extends well beyond what sleep deprivation alone explains.
Chronic inflammation impairs ferritin interpretation rather than causing true depletion – but it’s important for understanding ferritin results. Because ferritin is an acute phase reactant, inflammatory conditions elevate ferritin production independent of iron stores. A person with significant chronic inflammation – obesity-related, autoimmune, or infectious – may have ferritin that appears adequate (40-80 ng/mL) while having functionally depleted iron available for use, because inflammatory signals are simultaneously inflating ferritin and suppressing iron release through hepcidin elevation. When hs-CRP is elevated alongside ferritin, the ferritin value overstates true iron storage status and must be interpreted with this caveat.
What Causes High Ferritin?
Elevated ferritin above 200-300 ng/mL in otherwise healthy individuals always warrants investigation to distinguish true iron overload from inflammatory elevation.
Hereditary hemochromatosis is the most common serious genetic cause of elevated ferritin in populations of Northern European descent. HFE gene mutations – particularly the C282Y variant – cause inappropriate upregulation of intestinal iron absorption, progressively loading iron into the liver, heart, pancreas, and joints over decades. Ferritin rises progressively over years, often reaching hundreds or thousands of ng/mL before organ damage becomes clinically apparent. The classic presentation – liver disease, diabetes, arthropathy, cardiac disease, and skin bronzing – occurs after decades of iron accumulation. Ferritin and transferrin saturation screening can identify hemochromatosis long before organ damage accrues, making monitoring genuinely lifesaving. Elevated ferritin combined with transferrin saturation above 45-50% should prompt HFE genetic testing.
Chronic inflammation is the most common cause of modestly elevated ferritin (100-400 ng/mL) in people without iron overload. Because ferritin is an acute phase reactant, any sustained inflammatory state – obesity, metabolic syndrome, autoimmune conditions, chronic infections, inflammatory bowel disease – drives ferritin production upward through inflammatory cytokine signaling, independent of iron stores. Distinguishing inflammatory ferritin elevation from true iron overload requires assessing transferrin saturation: in true iron overload, transferrin saturation is high (above 45%); in inflammatory ferritin elevation without iron overload, transferrin saturation is typically normal or low.
Non-alcoholic fatty liver disease (NAFLD) and alcoholic liver disease both cause ferritin elevation through liver cell damage and inflammatory signaling. Liver cells contain the highest ferritin concentrations in the body – liver damage releases intracellular ferritin into the bloodstream, elevating serum levels. Elevated ferritin in the setting of obesity, metabolic syndrome, or alcohol use should prompt liver function assessment.
Metabolic syndrome consistently produces elevated ferritin through a combination of inflammatory mechanisms, insulin resistance-related iron dysregulation, and subclinical fatty liver. Ferritin reduction in metabolic syndrome often follows improvement in metabolic health markers rather than requiring iron-specific intervention.
Excessive iron supplementation without confirmed deficiency or without monitoring builds iron stores progressively. Because the body has limited iron excretion capacity, supplemental iron taken beyond what’s needed for repletion accumulates. This is the most straightforward preventable cause of iron overload and underscores why supplementation should be guided by testing.
Hemolytic conditions – where red blood cells break down prematurely – release hemoglobin that is processed into ferritin, elevating levels while actual iron utilization may be impaired.
How to Optimize Ferritin
Ferritin optimization follows directly from understanding its causes – whether your ferritin is too low, appropriately elevated from true iron overload, or inflated by inflammation determines the entire intervention strategy.
For low ferritin – dietary optimization first. Prioritize heme iron sources with the highest bioavailability – red meat 3-5 times weekly, organ meats like liver once or twice weekly for people willing to include them (beef liver contains roughly 6 mg highly bioavailable heme iron per 100g), shellfish particularly oysters and clams, and dark poultry meat. Pair non-heme iron sources – lentils, white beans, tofu, pumpkin seeds, dark leafy greens – with vitamin C-rich foods at the same meal to meaningfully enhance non-heme iron absorption.
Strategically separate iron-rich meals from absorption inhibitors. Coffee and tea consumed with meals reduce non-heme iron absorption by 50-90% through polyphenol binding. Calcium from dairy or supplements competes directly with iron for intestinal transport. Consuming these foods and drinks between meals rather than with iron-rich meals can meaningfully improve net iron absorption from the same dietary intake.
Supplement when diet isn’t closing the gap. When ferritin is below 50 ng/mL and dietary optimization is insufficient, iron supplementation is appropriate and often necessary. Ferrous bisglycinate (iron chelated to glycine) is generally preferred over ferrous sulfate for its improved absorption, lower required dose, and substantially fewer gastrointestinal side effects – constipation and nausea that often cause people to abandon iron supplementation are significantly less common with bisglycinate forms. Typical supplemental doses of 25-50 mg elemental iron daily or every other day – the latter showing favorable absorption kinetics due to hepcidin cycling – are appropriate starting points, but physician guidance based on your specific ferritin level and situation is the right approach.
Take iron supplements with vitamin C (250-500 mg) to enhance absorption. Take them separately from coffee, tea, calcium supplements, and antacids. Avoid taking with meals that contain significant dairy, legumes, or whole grains unless paired with vitamin C.
Monitor ferritin every 2-3 months during repletion. Ferritin rises gradually – expect 4-8 weeks to see meaningful increases and 3-6 months to fully replete from significantly depleted levels. Monitoring ensures you’re responding appropriately and prevents overshooting into excess.
Address root causes alongside supplementation. Supplementing iron without addressing why ferritin is low often results in temporary improvement followed by recurrence. Evaluate for heavy menstrual bleeding and discuss management options. Test for H. pylori if absorption seems impaired. Assess for celiac disease if iron deficiency is severe or refractory. Investigate gastrointestinal bleeding sources when clinically indicated. Reduce training volume temporarily if overtraining is the primary driver.
For elevated ferritin from inflammation – treat the underlying cause. If ferritin is elevated with normal transferrin saturation and elevated hs-CRP, the priority is identifying and addressing the inflammatory driver – whether metabolic, autoimmune, infectious, or hepatic. Iron restriction or therapeutic phlebotomy is not appropriate for inflammation-driven ferritin elevation.
For true iron overload from hemochromatosis – therapeutic phlebotomy. Regular removal of whole blood units depletes excess iron stores gradually and safely, reducing ferritin and organ iron burden over months to years. This is the primary treatment for hereditary hemochromatosis and is highly effective when initiated before significant organ damage occurs. Maintaining ferritin in the 50-100 ng/mL range through periodic phlebotomy dramatically reduces the risk of hemochromatosis complications.
Ferritin and Other Health Markers
Ferritin tells its most complete story when interpreted alongside related markers that reveal the full iron and inflammatory picture.
Serum iron and transferrin saturation are the essential companions to ferritin. Low ferritin with low transferrin saturation (below 20%) and low-to-normal serum iron confirms iron deficiency as the diagnosis. Normal or high ferritin with high transferrin saturation (above 45%) points toward iron overload. Normal ferritin with low transferrin saturation suggests functional iron deficiency from inflammation – iron is present in stores but not being released effectively. Each combination tells a different story requiring a different response.
TIBC (total iron binding capacity) rises in iron deficiency – the body upregulates transport protein production trying to capture more iron from a depleted supply – and falls in iron overload as binding sites become saturated. Rising TIBC alongside falling ferritin confirms iron depletion even when ferritin is still technically within the reference range.
Hemoglobin and hematocrit reflect the downstream consequence of iron status. Normal hemoglobin with low ferritin confirms the pre-anemic iron depletion phase – the phase with the greatest opportunity for intervention before significant functional decline.
hs-CRP is essential for interpreting ferritin correctly. Elevated hs-CRP (above 1.0 mg/L) alongside elevated ferritin shifts the differential toward inflammatory ferritin elevation rather than true iron overload. Elevated hs-CRP alongside borderline ferritin means actual iron stores may be more depleted than ferritin reflects, because inflammation is inflating the ferritin value.
Transferrin saturation above 45% combined with elevated ferritin should always prompt HFE genetic testing to evaluate for hereditary hemochromatosis.
Thyroid markers (TSH, free T3, free T4) are worth assessing alongside ferritin when thyroid symptoms are present, given iron’s role in thyroid hormone synthesis. Low ferritin impairing thyroid peroxidase activity can produce thyroid symptoms without primary thyroid pathology.
Vitamin B12 and folate are relevant when ferritin is being assessed in the context of fatigue and reduced performance – B12 and folate deficiency independently impair red blood cell production and energy metabolism, and deficiencies can coexist with iron deficiency, each contributing to the symptom picture.
Frequently Asked Questions
What ferritin level is considered optimal?
For general health and performance, optimal ferritin is 70-150 ng/mL for both men and women. For active individuals engaging in regular moderate-to-intense exercise, targeting 100-150 ng/mL provides more robust reserves given higher iron turnover. For competitive endurance athletes, many sports medicine practitioners target 100-175 ng/mL. The standard laboratory reference range floor of 12-15 ng/mL represents the clinical deficiency threshold – not an optimization target.
Can ferritin be low even if my hemoglobin is normal?
Yes – and this is the most important and most commonly missed clinical scenario. Ferritin falls first as iron stores deplete, while hemoglobin remains normal throughout the iron depletion phase and often through the subsequent iron deficiency phase. Symptoms – fatigue, reduced exercise capacity, brain fog, hair loss – typically appear when ferritin falls below 30-50 ng/mL despite normal hemoglobin. This is why ferritin is the critical marker for iron assessment, not hemoglobin.
How do I know if my high ferritin is from inflammation or iron overload?
Check transferrin saturation alongside ferritin. In iron overload, transferrin saturation is typically elevated (above 45%) because the iron transport system is saturated with excess iron. In inflammatory ferritin elevation, transferrin saturation is typically normal or low because iron is being sequestered from circulation rather than accumulating in transport. Check hs-CRP to assess systemic inflammation. If transferrin saturation is elevated above 45% with elevated ferritin, pursue HFE genetic testing to evaluate for hereditary hemochromatosis.
Why do I still have symptoms if my ferritin is in the normal range?
Because normal range doesn’t mean optimal range. A ferritin of 20-40 ng/mL is technically within the standard reference range on most lab reports but represents depleted iron stores insufficient for optimal cellular function. Research consistently shows that symptoms of functional iron deficiency appear below 30-50 ng/mL despite normal hemoglobin. If your ferritin is low-normal and you have symptoms consistent with iron deficiency, repletion to the 70-150 ng/mL range through diet and supplementation is a reasonable therapeutic trial.
How long does it take to raise ferritin levels?
Ferritin rises more slowly than hemoglobin in response to iron repletion. With appropriate supplementation (25-50 mg elemental iron daily or every other day), expect ferritin to rise 5-15 ng/mL per month depending on the degree of deficiency, supplementation dose, absorption efficiency, and ongoing iron losses. Moving ferritin from 15 ng/mL to 100 ng/mL typically requires 4-6 months of consistent supplementation. Symptoms often improve before ferritin reaches optimal range, but continuing until stores are fully replenished prevents rapid recurrence.
Should women have different ferritin targets than men?
Women’s ferritin naturally runs lower than men’s in the reproductive years due to menstrual iron losses – average ferritin in premenopausal women is 25-50 ng/mL compared to 75-150 ng/mL in age-matched men. But lower average ferritin doesn’t mean lower optimal ferritin. The performance and health evidence supports the same optimization targets for both sexes – 70-150 ng/mL for general health, 100-150+ ng/mL for active individuals. The practical implication is that most premenopausal women need deliberate dietary iron emphasis and often supplementation to achieve optimal ferritin, while most men can maintain adequate stores through diet alone.
Is it dangerous to take iron supplements if my ferritin is already normal?
Yes – iron supplementation without confirmed deficiency risks progressive iron accumulation and overload. The body has limited iron excretion capacity, so excess supplemental iron is stored in tissues over time. People with hereditary hemochromatosis are particularly vulnerable – supplementing iron without knowing your HFE status when ferritin is already normal or elevated could accelerate iron loading significantly. Always confirm iron status through ferritin and transferrin saturation before starting supplementation, and monitor during supplementation.
Can ferritin affect mood and mental health?
Directly, yes. Iron is required for the synthesis of dopamine, serotonin, and norepinephrine – the primary neurotransmitters governing mood, motivation, and emotional regulation. Depleted ferritin impairs these synthesis pathways independently of anemia, producing symptoms including low mood, reduced motivation, emotional flatness, irritability, and anxiety that improve with ferritin repletion. People receiving psychiatric diagnoses or medication for mood disorders without having comprehensive iron assessment may be addressing symptoms while missing a straightforward contributing cause.
Testing Ferritin With ApexBlood
ApexBlood’s comprehensive blood panel includes ferritin alongside the complete iron panel – serum iron, TIBC, transferrin saturation, hemoglobin, and hematocrit – providing the full context needed to interpret ferritin correctly rather than in isolation.
A ferritin number without transferrin saturation, serum iron, and an inflammatory marker tells an incomplete story. Is depleted ferritin driving your fatigue, or is normal ferritin being inflated by inflammation while functional iron availability is actually impaired? Is elevated ferritin reflecting iron overload that requires investigation, or is it an acute phase response to chronic metabolic inflammation? The surrounding data answers these questions.
Real physician consultation – not automated reports or algorithm-generated recommendations – means your iron markers are interpreted in the context of your complete biological picture, your symptoms, your activity level, and your goals. That’s the difference between a number and an action plan.
Most physicians flag ferritin only when it falls below their lab’s reference range floor. High performers understand that the gap between the reference range floor and the optimal range is where most of the performance-relevant iron deficiency lives – and that catching ferritin depletion before it reaches clinical significance is exactly where the value of proactive testing lies.
Get comprehensive testing – $189
The Bottom Line on Ferritin
Ferritin is the most important iron marker in routine blood testing – the earliest to shift in iron depletion, the most predictive of functional iron deficiency symptoms, and the most actionable target for optimization. Yet it’s routinely misinterpreted by applying a reference range floor that has nothing to do with optimal function.
The standard laboratory lower limit of 12-15 ng/mL represents the edge of clinical disease. Optimal ferritin for performance, cognitive function, energy, hair retention, thyroid support, and immune resilience is 70-150 ng/mL – with active individuals and athletes targeting 100-175 ng/mL for robust iron reserves that support high physiological demand.
The gap between 15 ng/mL and 100 ng/mL isn’t just a number on a lab report. It’s the difference between exhaustion and energy, between brain fog and clarity, between hair that thins and hair that thrives, between workouts that plateau and performance that improves. It’s a gap that standard medicine routinely ignores and that comprehensive testing reveals.
Ferritin depletes silently. Symptoms precede anemia by months to years. Repletion takes time, requires strategy, and demands addressing root causes rather than just supplementing around them. And elevated ferritin carries its own risks – hereditary hemochromatosis is common, underdiagnosed, and preventable when caught through monitoring rather than discovered after organ damage accumulates.
High performers don’t wait for hemoglobin to drop before addressing iron status. They measure ferritin proactively, understand what the number actually means relative to optimal function rather than clinical disease thresholds, and act on the gap between where they are and where their biology needs to be.
You can’t optimize what you don’t measure. Stop accepting reference range floors as performance targets – they were never designed to be.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Ferritin levels and iron status require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.