
Globulins are the second-largest protein fraction in your blood after albumin, and they encompass an enormously diverse group of proteins – including all your antibodies (immunoglobulins), complement proteins, transport proteins, clotting factors, and acute phase reactants. While albumin reflects your liver’s protein-making capacity and your nutritional status, globulins primarily reflect your immune system’s activity level. Elevated globulins can signal chronic infection, autoimmune disease, liver disease, or in more serious cases, blood cancers like multiple myeloma. Low globulins can indicate immune deficiency. Globulin is most valuable when broken down further into its component fractions through serum protein electrophoresis – but even the total globulin level, calculated from total protein minus albumin, provides meaningful initial insight that too often goes unexplained on routine lab reports.
What Are Globulins?
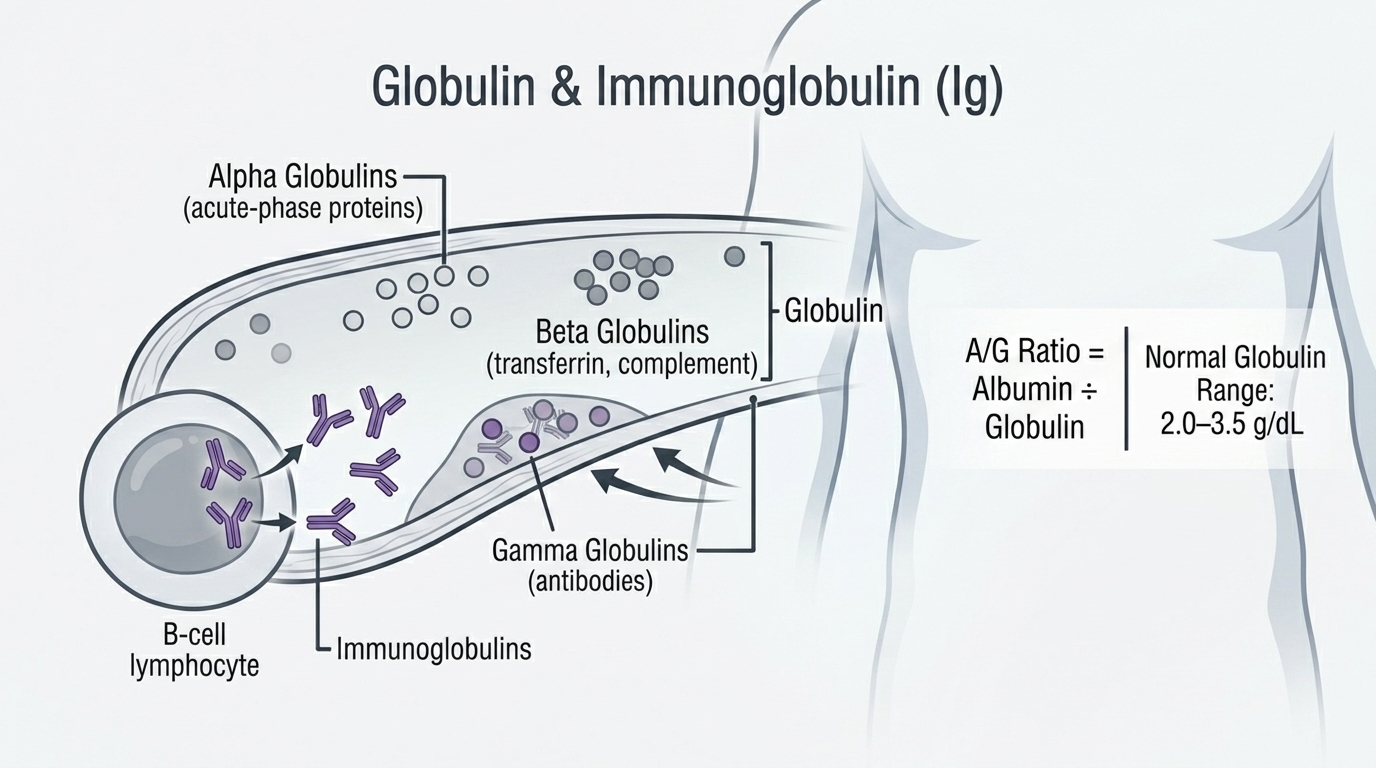
Globulin is not a single protein but rather a heterogeneous group of proteins separated from albumin during protein electrophoresis. They are divided into four major fractions. Alpha-1 globulins include alpha-1 antitrypsin (which protects lung tissue from neutrophil elastase) and other acute phase proteins. Alpha-2 globulins include haptoglobin, ceruloplasmin (copper carrier), and alpha-2 macroglobulin. Beta globulins include transferrin (iron transporter), complement proteins, LDL cholesterol carrier (apolipoprotein B), and some immunoglobulins. Gamma globulins are predominantly immunoglobulins (IgG, IgA, IgM, IgE, IgD) – the antibodies produced by plasma cells that form the adaptive immune response.
The serum globulin reported on a basic panel is the calculated total of all these fractions: Total Protein minus Albumin. A high globulin therefore means one or more of these fractions is elevated above the expected level. Knowing which fraction is elevated requires serum protein electrophoresis (SPEP), which separates the fractions visually and identifies whether any elevation is polyclonal (broad, reflecting immune activation from multiple plasma cell clones) or monoclonal (a sharp spike from a single clone – an M-spike – which raises concern for multiple myeloma or related disorders).
Why Globulins Matter for Performance and Health
Globulins matter primarily as indicators of immune system state. Chronically elevated globulins from persistent immune activation – whether from unresolved infections, autoimmune activity, chronic inflammation, or smoldering blood cancers – represent a biological burden that affects energy, recovery, and long-term health. The immune system’s constant engagement with a chronic trigger consumes resources, generates inflammatory mediators, and over time contributes to the accelerated aging and organ damage associated with chronic inflammation.
For high performers, persistently elevated globulins in the absence of an obvious cause should prompt investigation rather than reassurance. A globulin above 3.5-4.0 g/dL that is dismissed as “just slightly elevated” could be the first visible signal of an autoimmune condition in early stages, a chronic infection yet to produce obvious symptoms, or a plasma cell dyscrasia that is far more manageable when caught early than when identified after significant disease progression.
Normal vs. Optimal Globulin Levels
Standard Reference Ranges: Most laboratories report globulin (calculated) as normal between 2.0 and 3.5 g/dL, or sometimes 1.5-4.0 g/dL depending on the laboratory. The A/G ratio (albumin divided by globulin) is also calculated, with a normal ratio of approximately 1.2-2.2.
The Problem With “Normal”: Globulin at 2.1 g/dL and 3.4 g/dL are both “normal.” In context with albumin and A/G ratio, they paint different pictures. Globulin at 3.4 g/dL alongside albumin at 3.8 g/dL produces an A/G ratio below 1.0 – a low A/G that raises concern for liver disease or chronic immune activation even when total protein appears normal. The diagnosis of multiple myeloma and related disorders is notoriously delayed – often by years – because mildly elevated total protein or globulin is dismissed when it first appears on routine labs. Any upward trend in globulins over serial measurements deserves attention.
Optimal Globulin: For most healthy adults, globulin in the range of 2.0-3.0 g/dL alongside normal albumin (above 4.0 g/dL) and A/G ratio above 1.5 reflects a healthy immune and protein status. Globulin consistently above 3.5 g/dL warrants investigation. Globulin below 2.0 g/dL warrants evaluation for immune deficiency or protein malnutrition.
What Causes High Globulins?
Chronic infections are a major cause – HIV, hepatitis B, hepatitis C, tuberculosis, malaria, and chronic bacterial infections all stimulate persistent immunoglobulin production, elevating gamma globulins polyclonally. Autoimmune diseases including lupus, rheumatoid arthritis, Sjogren’s syndrome, and primary biliary cholangitis drive polyclonal gamma globulin elevation through chronic immune activation. Chronic liver disease (cirrhosis) characteristically produces elevated gamma globulins alongside falling albumin – a pattern called beta-gamma bridging on protein electrophoresis. Multiple myeloma, Waldenstrom macroglobulinemia, and other plasma cell dyscrasias produce monoclonal immunoglobulin elevation (M-spike) that appears as a sharp peak on SPEP. Sarcoidosis, inflammatory bowel disease, and other inflammatory conditions can elevate alpha and beta globulin fractions as part of the acute phase response. Dehydration concentrates all proteins including globulins.
What Causes Low Globulins?
Primary immunodeficiency disorders including common variable immunodeficiency (CVID) and agammaglobulinemia cause low or absent immunoglobulins (hypogammaglobulinemia) from impaired antibody production. This manifests as low globulins and very low or absent gamma fraction on SPEP. Secondary immunodeficiency from chemotherapy, immunosuppressive medications (corticosteroids, biologic agents), HIV/AIDS with advanced immune depletion, and bone marrow suppression can all lower globulins. Protein-losing enteropathy and nephrotic syndrome cause loss of all protein fractions including globulins. Severe malnutrition impairs all protein synthesis. Neonates normally have low globulin (their immune system is immature) – this normalizes as the immune system develops through childhood.
The A/G Ratio and What It Reveals
The albumin-to-globulin (A/G) ratio – the most clinically useful calculation derived from globulin measurement – should normally be above 1.0 (albumin should exceed globulin). A reversed A/G ratio (below 1.0) means globulins have risen above albumin – a pattern classically associated with chronic liver disease, chronic infection, and autoimmune disease where globulins are high and albumin is falling. A very high A/G ratio (above 2.5-3.0) with high albumin and very low globulins raises concern for immune deficiency. For high performers, a declining A/G ratio trend over serial labs – even while individual values remain technically within range – is a meaningful signal worth tracking and investigating.
Frequently Asked Questions
What does elevated globulin mean on a blood test?
Elevated total globulin (above 3.5-4.0 g/dL) means your immune system is producing more antibodies or acute phase proteins than expected. The most common causes are chronic infections, autoimmune conditions, chronic liver disease, and inflammatory states. More rarely, it signals a plasma cell dyscrasia like multiple myeloma. Any persistent globulin elevation should prompt SPEP to determine whether the elevation is polyclonal (broad, usually infection or inflammation) or monoclonal (a single sharp peak, requiring further workup).
When should I get serum protein electrophoresis (SPEP)?
SPEP should be considered whenever globulin is elevated without a clear explanation, whenever total protein is above 9 g/dL, whenever there is unexplained weight loss or bone pain alongside high protein, or when multiple myeloma or related disorders are being investigated. SPEP is also used to monitor known plasma cell dyscrasias. It is a relatively inexpensive and highly informative test that can identify monoclonal protein production years before multiple myeloma becomes symptomatic.
Can diet affect globulin levels?
Diet has limited direct effects on globulin levels. Anti-inflammatory dietary patterns that reduce chronic inflammatory burden – emphasizing omega-3 rich foods, vegetables, minimizing processed foods and refined carbohydrates – can gradually lower elevated globulins driven by inflammation. Adequate dietary protein supports normal immunoglobulin production. But direct dietary manipulation of globulin levels is not a reliable short-term intervention – the primary drivers are immune activation states, infections, and disease processes rather than nutrition per se.
Is a low A/G ratio always a concern?
A low A/G ratio (below 1.0) is always worth investigating rather than dismissing. The most common causes are liver disease (falling albumin), chronic infection or autoimmune disease (rising globulins), or a combination. A ratio between 1.0 and 1.2 warrants attention but is less urgent. The trend over time matters – a declining A/G ratio across multiple lab results suggests a progressive process worth identifying even if individual values are technically within normal limits.
Testing Globulin With ApexBlood
Globulin is calculated and reported in ApexBlood’s comprehensive panel alongside albumin, total protein, A/G ratio, and liver function markers. When globulin is elevated without obvious explanation, our physicians can guide appropriate follow-up including SPEP and targeted infection or autoimmune screening. Interpreting globulin in the context of your full metabolic and immune picture is how you go from a number to an actionable insight.
Get comprehensive testing for $189
The Bottom Line on Globulin
Globulin is your immune system’s fingerprint in your bloodstream. When it is elevated, it tells you the immune system is activated – and the question is why. Chronic infection, autoimmune disease, liver disease, and blood cancers all leave their mark on the globulin fraction. A gradually rising globulin or declining A/G ratio on serial labs is not background noise to dismiss – it is a biological trend worth investigating before it progresses to something harder to treat. Stop accepting “slightly elevated globulin, nothing to worry about” without understanding what is driving it. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Globulin levels and immune status require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.