
HDL Cholesterol: Why “Good” Cholesterol Is Your Best Defense Against Heart Disease
Understanding HDL’s protective role and how to optimize your levels for cardiovascular health
What Is HDL Cholesterol?
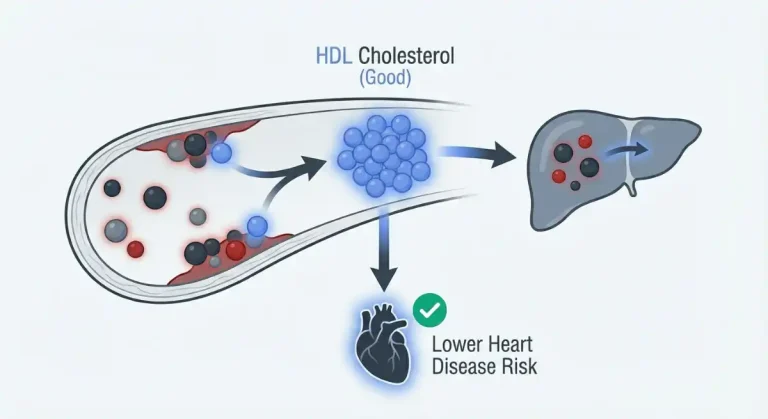
HDL cholesterol stands for high-density lipoprotein cholesterol, commonly known as “good” cholesterol. Unlike other forms of cholesterol that can accumulate in arterial walls and increase heart disease risk, HDL actively protects your cardiovascular system through a process called reverse cholesterol transport.
HDL particles travel through your bloodstream acting as cholesterol scavengers. They pick up excess cholesterol from arterial walls, tissues, and other lipoproteins, then transport it back to your liver for processing and elimination from your body. This continuous removal of cholesterol from places where it can cause harm is why HDL is considered protective rather than harmful.
The “high-density” in the name refers to the particle structure. HDL particles contain more protein relative to lipid compared to other lipoproteins, making them denser. This structural difference reflects their unique function in cholesterol transport and metabolism.
Higher HDL levels correlate with lower cardiovascular disease risk across numerous studies. People with naturally elevated HDL (through genetics or lifestyle) experience fewer heart attacks and strokes. Conversely, low HDL is an independent risk factor for cardiovascular disease, even when other cholesterol markers appear normal.
Understanding your HDL level is essential for cardiovascular optimization. While lowering LDL cholesterol gets most of the attention in conventional medicine, raising HDL often provides equal or greater cardiovascular protection, particularly for those focused on long-term health and longevity.
Why HDL Cholesterol Matters for Cardiovascular Health
HDL performs multiple protective functions that extend beyond simple cholesterol removal, making it one of the most important cardiovascular health markers.
Reverse Cholesterol Transport
The primary function of HDL is removing cholesterol from peripheral tissues and arterial walls. When cholesterol accumulates in artery walls, it contributes to atherosclerotic plaque formation. HDL directly counteracts this process by constantly clearing excess cholesterol before it can cause damage.
Think of HDL as your cardiovascular cleaning crew. The more HDL you have, the more efficiently your body removes cholesterol from places where it doesn’t belong. Low HDL means inadequate cleaning capacity, allowing cholesterol to accumulate over time.
Anti-Inflammatory Effects
HDL particles have anti-inflammatory properties independent of cholesterol transport. They reduce inflammatory cytokines and protect against oxidative stress, both of which accelerate atherosclerosis. Higher HDL levels correlate with lower systemic inflammation and better overall cardiovascular health.
Inflammation plays a central role in cardiovascular disease progression. Cholesterol in arterial walls becomes particularly problematic when it’s oxidized by inflammatory processes. HDL helps prevent both the accumulation and oxidation of arterial cholesterol.
Endothelial Function
The endothelium (the inner lining of blood vessels) is critical for cardiovascular health. HDL supports endothelial function by promoting nitric oxide production, which keeps blood vessels flexible and responsive. Better endothelial function means healthier, more resilient arteries.
Low HDL is associated with endothelial dysfunction, an early marker of cardiovascular disease that precedes obvious structural changes in arteries. Optimizing HDL helps maintain the health of your vascular system at the cellular level.
Antioxidant Properties
HDL particles carry enzymes that neutralize oxidized lipids, protecting LDL cholesterol from oxidation. Oxidized LDL is far more damaging to arterial walls than native LDL. By preventing LDL oxidation, HDL reduces one of the key drivers of atherosclerosis.
This antioxidant function represents another mechanism through which HDL protects cardiovascular health beyond simple cholesterol removal.
Normal vs. Optimal HDL Cholesterol Levels
Understanding where your HDL falls on the risk spectrum requires looking beyond basic “normal” ranges to true optimization targets.
Standard Reference Ranges
Most labs categorize HDL cholesterol as follows:
Men:
- Low (increased risk): Less than 40 mg/dL
- Normal: 40-60 mg/dL
- High (protective): Greater than 60 mg/dL
Women:
- Low (increased risk): Less than 50 mg/dL
- Normal: 50-60 mg/dL
- High (protective): Greater than 60 mg/dL
Women naturally have higher HDL levels than men on average, which partially explains their lower cardiovascular disease risk before menopause. The different thresholds reflect these natural differences.
The Problem With “Normal”
Having HDL in the “normal” range doesn’t mean you’re optimized. A man with HDL of 45 mg/dL is technically above the low threshold but still has substantially elevated cardiovascular risk compared to someone with HDL of 65 mg/dL.
These reference ranges are designed to identify obvious deficiency, not optimal function. Many people with HDL in the “normal” range would benefit significantly from raising it higher.
Optimal Range for Performance and Longevity
For high performers focused on cardiovascular optimization:
Men:
- Optimal: Greater than 60 mg/dL
- Excellent: 70-80 mg/dL
- Exceptional: Greater than 80 mg/dL
Women:
- Optimal: Greater than 70 mg/dL
- Excellent: 80-90 mg/dL
- Exceptional: Greater than 90 mg/dL
Higher is generally better for HDL, with no established upper limit of benefit for most people. The small percentage of individuals with extremely high HDL (over 100 mg/dL) due to genetic factors typically have excellent cardiovascular health, though rare genetic conditions can occasionally cause dysfunctional HDL at very high levels.
The goal is maximizing this protective lipoprotein. Every 1 mg/dL increase in HDL correlates with approximately 2-3% reduction in cardiovascular disease risk. Moving from 45 to 65 mg/dL can reduce your risk by 40-60%, a dramatic improvement for long-term health.
Symptoms and Consequences of Low HDL Cholesterol
Low HDL produces no immediate symptoms but significantly increases long-term cardiovascular disease risk. By the time symptoms of heart disease appear, substantial arterial damage has already occurred.
Increased Cardiovascular Disease Risk
Low HDL is an independent risk factor for heart disease. Even with normal or optimal LDL cholesterol, insufficient HDL substantially increases your risk of heart attack and stroke. The combination of low HDL with other risk factors (elevated LDL, high triglycerides, hypertension) creates multiplicative rather than additive risk.
Studies consistently show that low HDL predicts cardiovascular events more accurately than many other lipid markers. Someone with low HDL faces 2-3 times higher cardiovascular risk compared to someone with optimal levels, regardless of other factors.
Accelerated Atherosclerosis
Without adequate HDL to remove cholesterol from arterial walls, atherosclerotic plaque forms more rapidly. This process begins in your 20s and 30s but doesn’t produce symptoms until arteries are significantly narrowed or plaques rupture decades later.
Low HDL throughout your 30s and 40s allows silent arterial damage that manifests as heart attacks or strokes in your 50s and 60s. Prevention requires optimizing HDL long before symptoms develop.
Metabolic Dysfunction
Low HDL typically correlates with other metabolic problems including insulin resistance, elevated triglycerides, excess visceral fat, and metabolic syndrome. These issues work synergistically to increase cardiovascular risk beyond what any single marker suggests.
The presence of low HDL often indicates broader metabolic dysfunction requiring comprehensive intervention rather than just addressing lipids in isolation.
Increased Inflammation
Low HDL levels correlate with higher systemic inflammation. Without HDL’s anti-inflammatory effects, inflammatory processes proceed unchecked, accelerating arterial damage and increasing risk for numerous chronic diseases beyond just cardiovascular conditions.
What Causes Low HDL Cholesterol?
Understanding factors that suppress HDL allows for targeted optimization strategies.
Sedentary Lifestyle
Physical inactivity is one of the strongest predictors of low HDL. The relationship is dose-dependent: more sedentary time correlates with lower HDL, while more physical activity correlates with higher HDL.
Exercise stimulates enzymes involved in HDL production and metabolism. Without regular physical activity, these pathways become sluggish, and HDL production decreases. Even modest increases in activity can raise HDL noticeably within weeks to months.
Excess Body Fat and Visceral Adiposity
Carrying excess body fat, particularly visceral fat (belly fat), suppresses HDL production. The relationship is independent of total body weight. You can have normal BMI but elevated visceral fat and correspondingly low HDL.
Visceral adipose tissue is metabolically active, secreting inflammatory cytokines and hormones that interfere with lipid metabolism. As visceral fat increases, HDL typically decreases in a dose-dependent manner.
Poor Diet Quality
Dietary patterns high in refined carbohydrates and added sugars lower HDL while raising triglycerides. This creates a particularly unfavorable lipid profile from both directions.
Trans fats (now largely removed from food supply but still present in some processed foods) dramatically lower HDL. Even small amounts of trans fat intake can suppress HDL levels substantially.
Diets very low in fat (below 15-20% of calories) can also lower HDL, though this is less common with modern eating patterns. Some dietary fat is necessary for optimal HDL production.
Smoking
Tobacco use significantly lowers HDL cholesterol. Even moderate smoking can reduce HDL by 10-15%. The effect is dose-dependent: more smoking correlates with lower HDL.
Smoking also impairs HDL function, making existing HDL particles less effective at reverse cholesterol transport. Both the quantity and quality of HDL suffer with tobacco use.
Insulin Resistance and Metabolic Syndrome
Insulin resistance and metabolic syndrome are strongly associated with low HDL. The metabolic dysfunction characteristic of these conditions suppresses HDL production while often elevating triglycerides and LDL.
Improving insulin sensitivity through exercise, body composition optimization, and dietary quality typically raises HDL as metabolic health improves.
Hypothyroidism
Underactive thyroid function affects lipid metabolism, often lowering HDL while raising LDL and total cholesterol. Optimizing thyroid function frequently improves HDL levels without other interventions.
Medications
Certain medications lower HDL as a side effect. Beta blockers (used for blood pressure and heart conditions), benzodiazepines (used for anxiety), and anabolic steroids all suppress HDL. If you’re taking medications that lower HDL, work with your physician on strategies to mitigate this effect.
Genetic Factors
Genetics influence HDL levels substantially. Some people naturally produce more HDL, while others struggle to maintain adequate levels despite optimal lifestyle. Genetic factors don’t eliminate the benefit of lifestyle optimization but do affect your individual baseline and response to interventions.
How to Increase HDL Cholesterol
Raising HDL requires consistent lifestyle optimization focused on the factors that most strongly influence HDL production and metabolism.
Increase Physical Activity
Exercise is the most powerful intervention for raising HDL. Both aerobic exercise and resistance training improve HDL, with aerobic activity showing particularly robust effects.
Regular aerobic exercise (running, cycling, swimming, brisk walking) consistently raises HDL in most people. The dose-response relationship suggests more activity produces greater benefits, though even moderate amounts help. Aim for at least 150 minutes of moderate-intensity aerobic exercise weekly, or 75 minutes of vigorous-intensity activity.
High-intensity interval training (HIIT) may be particularly effective for raising HDL while providing time-efficient workouts. Alternating periods of intense effort with recovery appears to stimulate HDL production more than steady-state moderate exercise alone.
Resistance training contributes to metabolic health and body composition, which indirectly supports better HDL levels. While the direct effect on HDL may be more modest than aerobic exercise, the overall metabolic benefits make resistance training valuable for comprehensive cardiovascular optimization.
Consistency matters more than intensity for HDL improvement. Regular ongoing activity over months and years produces sustained HDL elevation. Sporadic intense efforts followed by inactivity produce minimal lasting benefit.
Optimize Body Composition
Reducing excess body fat, particularly visceral fat, raises HDL levels. Even modest fat loss (5-10% of body weight) can significantly improve HDL in those carrying excess fat.
The relationship is dose-dependent: more fat loss generally correlates with greater HDL improvements, though this plateaus at healthy body fat levels. You can’t lower body fat indefinitely to raise HDL, but optimizing body composition to healthy ranges provides substantial benefit.
Focus on sustainable approaches through reasonable caloric balance, adequate protein intake (supporting satiety and muscle preservation), and consistent training rather than extreme dieting that’s impossible to maintain long-term.
Improve Dietary Quality
Overall dietary patterns affect HDL more than individual nutrients or foods.
Reduce refined carbohydrates and added sugars. High sugar intake lowers HDL while raising triglycerides. Replacing refined carbohydrates with whole food sources improves HDL in most people.
Include healthy fats from sources like olive oil, avocados, nuts, seeds, and fatty fish. Omega-3 fatty acids from fish appear particularly beneficial for cardiovascular health and may support HDL function.
Moderate alcohol consumption (particularly red wine) is associated with higher HDL in observational studies. However, the relationship is complex, and alcohol has other health effects. If you drink moderately already, it may contribute to HDL levels. If you don’t drink, the potential HDL benefit alone doesn’t justify starting.
Stop Smoking
If you smoke, quitting is one of the most impactful interventions for raising HDL and improving overall cardiovascular health. HDL typically rises within weeks of smoking cessation and continues improving over months.
Improve Metabolic Health
Addressing insulin resistance and metabolic syndrome raises HDL as metabolic function improves. Interventions that improve insulin sensitivity (exercise, body composition optimization, dietary quality) typically raise HDL as a beneficial side effect.
If you have prediabetes or type 2 diabetes, optimizing blood sugar control often improves HDL levels alongside other metabolic improvements.
Optimize Thyroid Function
If thyroid function is suboptimal, addressing it often improves HDL without additional interventions. Comprehensive thyroid testing (not just TSH) reveals dysfunction that standard screening might miss.
HDL Cholesterol and Hormone Optimization
Several hormone optimization treatments can affect HDL levels, requiring monitoring and occasionally intervention to maintain optimal cardiovascular health.
Testosterone Replacement Therapy (TRT)
Testosterone replacement therapy in men typically lowers HDL cholesterol modestly, with reductions of 5-15% common. This is one of the few negative metabolic effects of TRT and requires monitoring.
The HDL reduction from TRT rarely causes problems if starting HDL is optimal (above 60 mg/dL). Someone beginning TRT with HDL of 70 mg/dL might see it decrease to 60-65 mg/dL, still well within the protective range.
However, men with borderline or low HDL before starting TRT need careful monitoring. If HDL starts at 45 mg/dL and drops to 35-40 mg/dL on TRT, cardiovascular risk increases despite the many benefits testosterone provides.
Strategies to mitigate TRT’s effect on HDL include maintaining consistent exercise (particularly aerobic activity), optimizing body composition, ensuring excellent dietary quality, and avoiding other factors that suppress HDL (smoking, excessive alcohol, sedentary behavior).
For most men, the cardiovascular and metabolic benefits of TRT (improved body composition, better insulin sensitivity, increased energy for exercise) outweigh the modest HDL reduction. But monitoring is essential to ensure HDL doesn’t drop to levels that significantly increase risk.
Hormone Replacement Therapy (HRT) for Women
Estrogen replacement in women typically raises HDL cholesterol, one of several cardiovascular benefits of HRT. This contributes to the protective cardiovascular effects of estrogen and partially explains why cardiovascular disease risk increases after menopause when estrogen declines.
Women on HRT usually see HDL increases of 5-15%, improving their already favorable lipid profile. This is one mechanism through which HRT may reduce cardiovascular disease risk in appropriately selected women.
Progesterone’s effects on HDL vary depending on the type used. Natural progesterone has minimal effect on HDL, while some synthetic progestins can lower HDL modestly. This is one reason bioidentical hormones are often preferred for HRT protocols.
HDL Cholesterol and Metabolic Optimization Treatments
Several treatments used for metabolic optimization and longevity can positively affect HDL levels.
GLP-1 Agonists (Semaglutide, Tirzepatide)
GLP-1 receptor agonists used for weight loss and metabolic optimization typically improve HDL cholesterol modestly as part of their broader beneficial metabolic effects.
The HDL improvement appears related to the weight loss and body composition changes these medications produce rather than direct effects on lipid metabolism. As patients lose fat (particularly visceral fat) and improve insulin sensitivity, HDL typically rises 5-15%.
The magnitude of HDL improvement correlates with the amount of weight loss achieved. Patients losing substantial weight on GLP-1 agonists often see meaningful HDL improvements alongside reductions in triglycerides and improvements in other cardiovascular risk markers.
Metformin
Metformin’s effects on HDL are generally neutral to modestly positive. While not prescribed specifically for lipid optimization, the metabolic improvements Metformin produces (better insulin sensitivity, reduced inflammation, improved glucose control) often correlate with small HDL increases of 2-5 mg/dL.
The cardiovascular benefits of Metformin extend beyond lipid effects through multiple mechanisms including improved endothelial function, reduced oxidative stress, and favorable effects on weight and body composition.
Sermorelin
Sermorelin and growth hormone optimization can improve lipid profiles including modest HDL increases in some individuals. The effects appear mediated through improved body composition, reduced visceral fat, and enhanced metabolic function rather than direct effects on lipid metabolism.
The magnitude and consistency of HDL improvement with Sermorelin varies between individuals, but the overall metabolic optimization these treatments provide typically supports cardiovascular health through multiple pathways beyond just HDL changes.
HDL Cholesterol and Other Health Markers
HDL doesn’t exist in isolation. Understanding how it relates to other markers provides complete cardiovascular risk assessment.
Triglycerides
HDL and triglycerides typically move in opposite directions. High triglycerides often coincide with low HDL, creating a particularly unfavorable lipid profile called atherogenic dyslipidemia. This pattern strongly predicts cardiovascular disease risk.
Interventions that raise HDL usually lower triglycerides simultaneously. Reducing refined carbohydrates, increasing exercise, and improving body composition benefit both markers.
LDL Cholesterol
While LDL gets most attention in cardiovascular disease prevention, HDL’s protective effects can partially offset LDL’s risks. Someone with moderately elevated LDL but excellent HDL faces lower actual risk than someone with optimal LDL but very low HDL.
The cholesterol/HDL ratio (total cholesterol divided by HDL) captures this balance and often predicts risk better than LDL alone.
Inflammatory Markers
HDL’s anti-inflammatory effects mean higher HDL often correlates with lower inflammatory markers like high-sensitivity C-reactive protein (hs-CRP). The combination of optimal HDL and low inflammation provides powerful cardiovascular protection.
Conversely, low HDL with elevated inflammation creates particularly high risk requiring comprehensive intervention.
Insulin and Glucose
Insulin resistance suppresses HDL while typically elevating triglycerides. Improving insulin sensitivity through lifestyle optimization raises HDL as metabolic health improves.
Monitoring fasting insulin alongside HDL provides insight into metabolic health that standard glucose testing alone might miss.
HDL Cholesterol: Frequently Asked Questions
Can HDL be too high?
For most people, higher HDL is better with no established upper limit of benefit. Extremely high HDL (above 100 mg/dL) is usually protective, though rare genetic conditions can occasionally cause dysfunctional HDL at very high levels. If your HDL is above 100 mg/dL, discuss with your physician to rule out rare genetic lipid disorders.
How long does it take to raise HDL?
HDL responds to lifestyle changes over weeks to months. Consistent exercise often raises HDL noticeably within 6-12 weeks. Body composition changes take longer but produce sustained improvements. Expect meaningful HDL increases within 3-6 months of consistent lifestyle optimization.
Why is my HDL low despite exercising regularly?
Genetics play a significant role in HDL levels. Some people have lower HDL despite optimal lifestyle due to genetic factors affecting HDL production and metabolism. This doesn’t mean lifestyle optimization isn’t valuable (it still provides benefits), but expectations should be realistic based on your genetic baseline. Other factors like diet quality, body composition, and metabolic health also matter beyond just exercise.
Should I take medication to raise my HDL?
Medications to raise HDL (niacin, fibrates) have limitations and side effects that often outweigh benefits. Recent studies suggest that artificially raising HDL with medications doesn’t provide the cardiovascular benefits that naturally high HDL confers. Lifestyle optimization should be the primary approach for most people.
Does HDL matter if my LDL is optimal?
Yes. HDL provides cardiovascular protection independent of LDL levels. Even with optimal LDL, low HDL increases risk substantially. Both markers matter for comprehensive cardiovascular health assessment.
Can losing weight lower HDL?
During active weight loss, HDL sometimes temporarily decreases as your body mobilizes fat stores and alters lipid metabolism. This is usually transient. Once weight stabilizes at a lower level with improved body composition, HDL typically rises above baseline. Focus on the long-term trajectory rather than temporary fluctuations during active fat loss.
Testing HDL Cholesterol With Apex
Understanding your HDL cholesterol is essential for cardiovascular optimization and long-term health. This single marker provides powerful insight into your cardiovascular protection and metabolic health.
Our comprehensive blood panel includes complete lipid analysis (total cholesterol, HDL, LDL, triglycerides, cholesterol/HDL ratio) alongside 100+ other biomarkers across hormones, metabolism, inflammation, and organ function. This provides complete context for understanding not just your HDL level, but the factors affecting it and implications for your overall cardiovascular health.
Testing costs $189 with results available in 3-5 business days. Every result is reviewed by licensed medical professionals who provide detailed interpretation focused on optimization, not just disease screening.
If your HDL is suboptimal, we connect you with medical professionals who understand cardiovascular optimization and can discuss comprehensive strategies for improvement. If you’re considering or currently using hormone optimization (TRT, HRT) or metabolic treatments, we monitor HDL to ensure these interventions support rather than compromise your cardiovascular health.
Get Comprehensive Testing – $189 | Schedule Free Consultation
The Bottom Line on HDL Cholesterol
HDL cholesterol is your cardiovascular defense system. Higher levels provide powerful protection against heart disease, stroke, and atherosclerosis through multiple mechanisms extending beyond simple cholesterol removal.
The standard medical approach often ignores HDL while focusing exclusively on lowering LDL. The optimization approach recognizes that raising HDL through exercise, body composition improvement, and metabolic health optimization provides cardiovascular protection that medications struggle to replicate.
Men should target HDL above 60 mg/dL, ideally 70-80 mg/dL or higher. Women should target above 70 mg/dL, ideally 80-90 mg/dL or higher. These levels provide substantial cardiovascular protection and correlate with excellent long-term health outcomes.
You can’t optimize what you don’t measure. If you haven’t tested HDL and tracked it over time as part of comprehensive cardiovascular health assessment, you’re missing one of the most important predictors of your long-term heart health.
Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Low HDL cholesterol and cardiovascular disease risk require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment of cardiovascular conditions.