
Insulin is the most underrated biomarker in standard medical care. While your doctor tests fasting glucose every year, they almost certainly never test fasting insulin — despite the fact that insulin becomes abnormal years, sometimes decades, before glucose does. Elevated fasting insulin is the earliest measurable sign of insulin resistance, the metabolic dysfunction underlying type 2 diabetes, cardiovascular disease, obesity, PCOS, and accelerated aging. Missing it means missing the window when intervention is easiest and most effective.
Understanding your insulin level isn’t just about diabetes prevention. Insulin is a master metabolic hormone that regulates fat storage, muscle growth, inflammation, hunger, energy balance, and cellular aging pathways. When insulin is chronically elevated — even with “normal” glucose — metabolic dysfunction is already underway. This is the biomarker that tells you what your glucose cannot.
What Is Insulin?
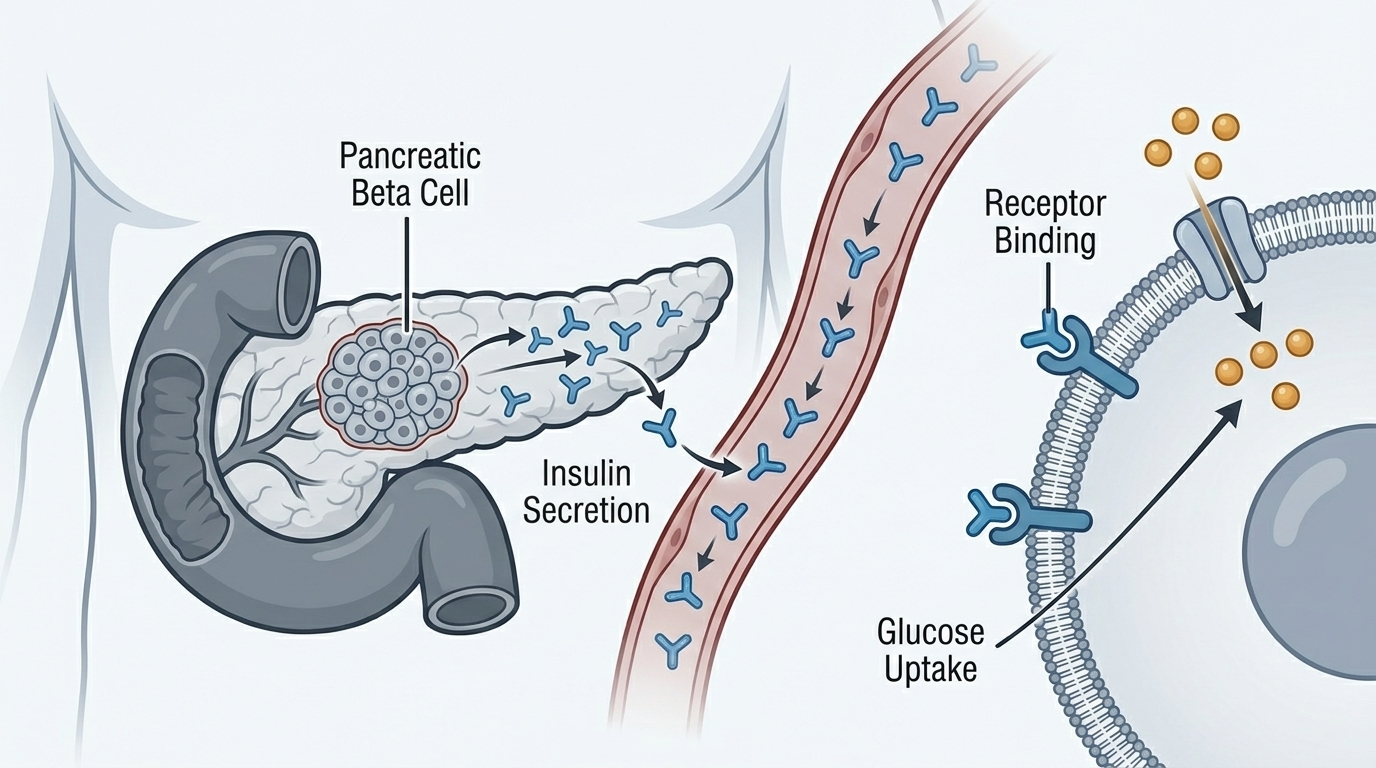
Insulin is a peptide hormone produced by beta cells in the pancreatic islets of Langerhans. Its primary function is to regulate blood glucose: when blood sugar rises after eating, the pancreas releases insulin, which signals cells throughout the body — primarily muscle, fat, and liver — to absorb glucose from the bloodstream. This drives blood glucose back down to baseline.
Beyond glucose regulation, insulin is a powerful anabolic hormone with wide-ranging effects. It promotes fat storage (by stimulating fat cells to absorb triglycerides and inhibiting lipolysis), drives muscle protein synthesis, regulates hunger signals, influences sex hormone binding globulin (SHBG) and therefore free testosterone levels, activates mTOR pathways (the cellular growth and protein synthesis signaling cascade), and suppresses autophagy (the cellular cleanup process linked to longevity).
A fasting insulin test measures insulin concentration in the blood after an overnight fast — when you haven’t eaten in 8–12 hours and insulin should be at its baseline. This reveals how much insulin your pancreas needs to produce just to maintain normal fasting glucose, which is the key indicator of insulin sensitivity.
Why Fasting Insulin Is the Early Warning Signal
Here’s the critical insight that most standard medical care misses: when cells become insulin resistant, the pancreas compensates by producing more insulin to achieve the same effect. For a long period — often years to decades — this compensation is successful. Glucose stays normal because the pancreas is working overtime. But insulin is elevated throughout this period, revealing the underlying dysfunction that glucose cannot yet detect.
By the time fasting glucose rises above 100 mg/dL (the prediabetic threshold), insulin resistance is typically well established and beta cell function may already be compromised. The window for easy lifestyle intervention has narrowed considerably. Testing fasting insulin catches the problem when it’s most reversible — when glucose still looks fine but insulin is already working too hard to keep it there.
Beyond disease prevention, chronically elevated insulin drives fat accumulation (insulin is the primary fat-storage hormone), impairs fat burning (high insulin suppresses lipolysis), increases inflammation, disrupts hormonal balance, promotes cellular aging through mTOR activation and autophagy suppression, and is associated with increased cancer risk through its growth-promoting effects.
Normal vs. Optimal Fasting Insulin Levels
Standard laboratory reference ranges for fasting insulin vary by lab but typically define “normal” as anywhere from 2 to 25 µIU/mL. This range is far too broad to be clinically useful for optimization — it was set to catch pathological extremes, not to define metabolic health.
Research-based optimal ranges are much tighter. Optimal fasting insulin for performance and longevity is below 8 µIU/mL, ideally below 5 µIU/mL. Fasting insulin above 10 µIU/mL strongly suggests early insulin resistance. Above 15 µIU/mL indicates significant insulin resistance requiring active intervention. Above 20 µIU/mL represents severe insulin resistance even if glucose appears normal.
The HOMA-IR (Homeostatic Model Assessment of Insulin Resistance) is a calculated index using fasting insulin and fasting glucose together: HOMA-IR = (Fasting Insulin × Fasting Glucose) ÷ 405. Optimal HOMA-IR is below 1.0; above 2.0 indicates insulin resistance; above 2.9 indicates significant insulin resistance. This combined calculation provides better insight than either marker alone.
What Causes High Fasting Insulin?
Elevated fasting insulin is primarily caused by insulin resistance — when cells require more insulin to achieve the same glucose-lowering effect. The root causes of insulin resistance include excess visceral (abdominal) adipose tissue, which releases inflammatory cytokines that directly impair insulin signaling; a diet consistently high in refined carbohydrates and added sugars, which chronically stimulates insulin secretion; physical inactivity and low muscle mass (muscle is the primary site of insulin-mediated glucose disposal); chronic sleep deprivation; chronic psychological stress with elevated cortisol; and certain medications.
Other causes of elevated insulin include insulinoma (a rare insulin-secreting pancreatic tumor), certain hypoglycemic medications, and reactive hypoglycemia. In women, PCOS (polycystic ovary syndrome) is strongly associated with insulin resistance and elevated insulin, creating a vicious cycle where high insulin drives androgen production, worsening the hormonal imbalance.
What Causes Low Fasting Insulin?
Very low fasting insulin (below 2 µIU/mL) can indicate type 1 diabetes or advanced type 2 diabetes with beta cell burnout — the pancreas can no longer produce adequate insulin. It can also be seen in people who are extremely lean and insulin sensitive, with very low-carbohydrate dietary patterns, or who have been fasting for extended periods. In the context of excellent metabolic health, low-normal insulin is ideal. In the context of high glucose, very low insulin suggests inadequate pancreatic function.
How to Optimize Your Insulin Levels
Improving insulin sensitivity — so that less insulin is required to manage blood glucose — is the primary goal. The most effective interventions are lifestyle-based and produce meaningful results within weeks to months.
Resistance training is uniquely powerful for insulin sensitivity because it builds muscle — the body’s largest glucose disposal organ. More muscle mass means more glucose can be cleared from the bloodstream with less insulin. Progressive resistance training 3–4 times weekly is among the most evidence-backed metabolic interventions available.
Reducing refined carbohydrate intake directly reduces insulin secretion demand. Replacing refined carbs with fiber, protein, and healthy fats lowers the glycemic load, reduces post-meal insulin spikes, and improves baseline insulin sensitivity over time. Very low carbohydrate or ketogenic diets produce the most dramatic rapid reductions in fasting insulin, though they’re not necessary for everyone.
Intermittent fasting or time-restricted eating reduces total insulin exposure by creating windows where insulin levels can fall to true baseline. Eating within a 6–10 hour window (rather than 12–16 hours) consistently shows improvements in fasting insulin and insulin sensitivity in clinical studies.
Weight loss, particularly visceral fat reduction, produces dramatic improvements in insulin sensitivity. Visceral fat is uniquely insulin-resistant and inflammatory — reducing it reliably improves insulin levels even with modest amounts of weight loss.
Medical Support for Insulin Optimization
When lifestyle optimization isn’t sufficient, medical interventions can meaningfully accelerate insulin sensitivity improvement. Metformin remains the gold standard pharmaceutical for insulin resistance, improving insulin sensitivity through multiple mechanisms and reducing fasting insulin levels. It’s safe, well-tolerated, inexpensive, and has longevity data behind it beyond its metabolic effects.
GLP-1 medications like semaglutide and tirzepatide improve insulin sensitivity significantly alongside their weight loss effects — visceral fat reduction directly reduces insulin resistance. In women, treating the underlying insulin resistance driving PCOS often requires combining lifestyle intervention with medical support. For men, chronically elevated insulin is associated with lower free testosterone (via increased SHBG and direct testicular suppression); addressing insulin resistance through lifestyle or hormone optimization often improves both metabolic and hormonal function simultaneously.
Getting your fasting insulin tested — alongside glucose, HbA1c, and a comprehensive metabolic panel — is the most important first step. See what ApexBlood tests to understand the full picture.
Frequently Asked Questions About Insulin
What is a normal fasting insulin level?
Laboratory “normal” ranges are typically 2–25 µIU/mL — far too broad to be useful for optimization. Research-based optimal fasting insulin is below 8 µIU/mL, ideally below 5 µIU/mL. Above 10 µIU/mL suggests early insulin resistance even with normal glucose; above 15 µIU/mL indicates significant insulin resistance requiring intervention.
Why does my doctor never test fasting insulin?
Standard care focuses on glucose as the primary marker for diabetes screening. Fasting insulin isn’t part of most routine panels despite being a far more sensitive early indicator of metabolic dysfunction. This is one of the core gaps that performance-focused blood testing addresses — testing insulin alongside glucose and HbA1c provides years of additional early warning that standard care misses entirely.
Can you have high insulin with normal glucose?
Yes — this is exactly the critical window that standard care misses. High insulin with normal glucose means insulin resistance is present but compensation is still working. Your pancreas is producing excess insulin to maintain normal glucose. This state can persist for years, driving fat accumulation, inflammation, and hormonal disruption, before glucose eventually rises. Catching it here means the most effective intervention window.
How does insulin affect weight loss?
Insulin is the primary fat-storage hormone. When insulin is elevated, fat burning is suppressed and fat storage is promoted — making weight loss extremely difficult regardless of caloric intake. High fasting insulin is a common hidden reason why people struggle to lose weight despite eating less and exercising more. Reducing insulin — through dietary changes, exercise, and when needed medical support — is often the missing piece that makes fat loss finally work.
Does fasting lower insulin?
Yes. Insulin secretion is primarily triggered by food intake, particularly carbohydrates. During a fast, insulin falls to its baseline level. Extended fasting or time-restricted eating reduces total daily insulin exposure, which over time improves insulin sensitivity. This is a significant mechanism behind the metabolic benefits of intermittent fasting approaches.
What is HOMA-IR and should I calculate it?
HOMA-IR (Homeostatic Model Assessment of Insulin Resistance) uses fasting insulin and glucose to calculate an insulin resistance index: (Fasting Insulin × Fasting Glucose) ÷ 405. Optimal is below 1.0; above 2.0 indicates insulin resistance; above 2.9 indicates significant insulin resistance. This combined index is more informative than either marker alone and is worth calculating whenever both are tested.
Is fasting insulin tested at ApexBlood?
Yes. Fasting insulin is included in ApexBlood’s comprehensive metabolic panel alongside glucose and HbA1c, providing the complete picture of your insulin sensitivity and metabolic health. This combination — unavailable in most routine annual physicals — gives you years of advance warning over standard care.
Test your insulin alongside 100+ biomarkers for $189. See what we test →
The Bottom Line on Insulin
Fasting insulin is arguably the most important metabolic biomarker your doctor isn’t testing. It reveals insulin resistance years before glucose rises, provides the earliest actionable warning of metabolic dysfunction, and explains many performance problems — stubborn fat, fatigue, brain fog, hormonal imbalance — that normal glucose levels can’t account for. Optimal fasting insulin is below 8 µIU/mL, ideally below 5. If yours is higher, the good news is that insulin resistance responds rapidly to the right interventions. The data starts with the test.
Medical Disclaimer: This information is for educational purposes only and does not constitute medical advice. Insulin levels and metabolic health require evaluation by qualified healthcare providers. Always consult licensed medical professionals for diagnosis and treatment.