
MCH – mean corpuscular hemoglobin – measures the average amount of hemoglobin packed inside each of your red blood cells. While MCV tells you about cell size and hemoglobin tells you the total amount of hemoglobin in your blood, MCH bridges both – showing whether individual cells are appropriately loaded with the oxygen-carrying protein that makes red blood cells functional. Low MCH means each red blood cell is carrying less hemoglobin than it should, reducing oxygen-carrying capacity per cell. High MCH occurs when cells are larger than normal and contain more hemoglobin as a result. MCH is rarely evaluated in isolation – it is most valuable as part of a complete red blood cell index analysis alongside MCV, MCHC, and ferritin – but it is a key piece of the puzzle in diagnosing why anemia is present and what nutritional or medical factor is causing it.
What Is MCH?
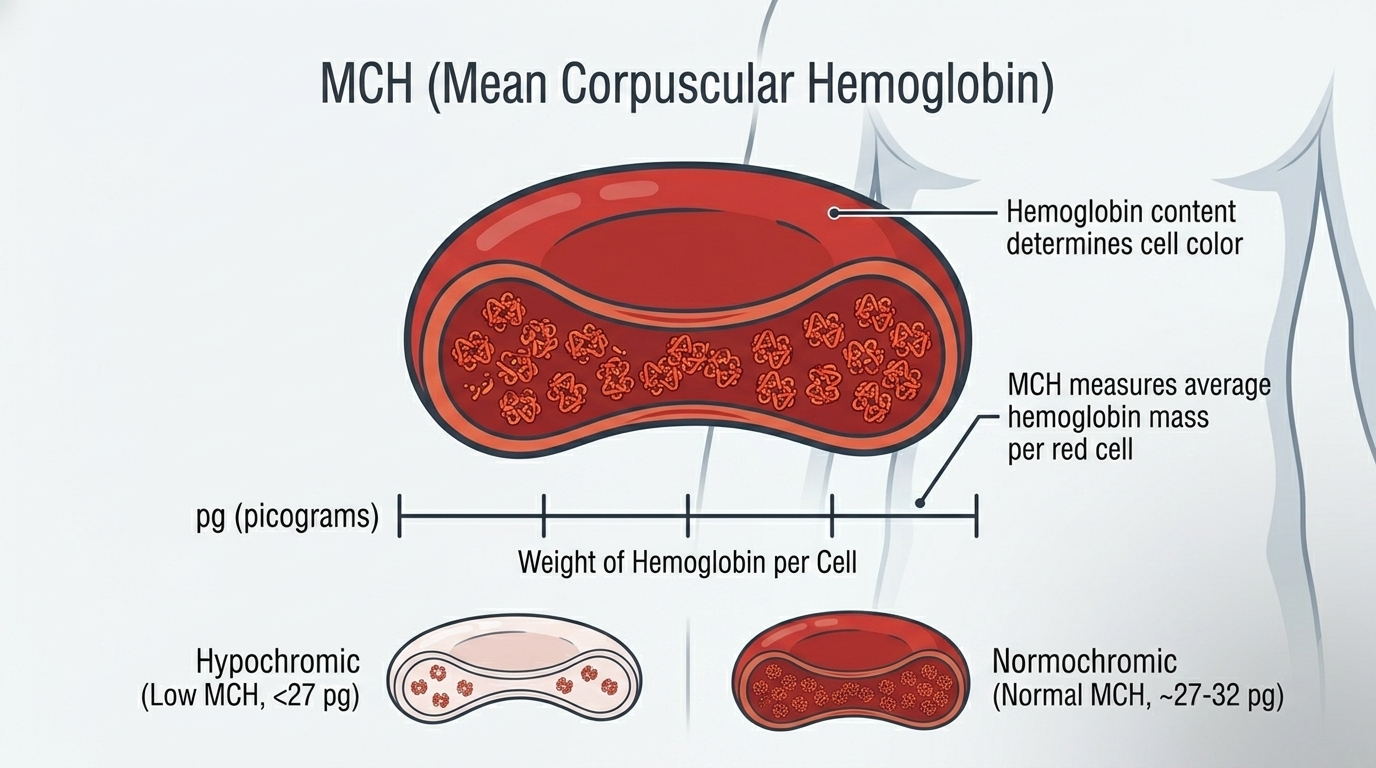
MCH stands for mean corpuscular hemoglobin. It represents the average mass of hemoglobin contained in a single red blood cell, measured in picograms (pg – one trillionth of a gram). Hemoglobin is the iron-containing protein that gives red blood cells their oxygen-carrying capacity and their characteristic red color. Each hemoglobin molecule contains four iron atoms, each capable of binding one oxygen molecule. A red blood cell contains approximately 270 million hemoglobin molecules, meaning each cell can theoretically carry over a billion oxygen molecules.
MCH is calculated from the complete blood count: it equals hemoglobin (in g/dL) divided by the red blood cell count (in millions per microliter), multiplied by 10. This calculation gives the average hemoglobin content per cell. Like MCV, MCH is reported automatically by hematology analyzers from the same measurement of hundreds of thousands of cells. Because hemoglobin content and cell volume are closely related (more hemoglobin requires more space), MCH and MCV tend to change in the same direction – low MCV and low MCH together characterize the classic iron-deficiency pattern.
Why MCH Matters for Oxygen Delivery and Performance
The functional purpose of red blood cells is oxygen delivery from the lungs to every tissue in the body – including working muscles during exercise. MCH is directly related to how much oxygen each individual red blood cell can transport. When MCH is low, each cell delivers less oxygen per pass through the circulation. The body compensates by increasing heart rate and cardiac output, but this compensation has limits – and in demanding situations like high-intensity exercise or altitude exposure, the deficit in oxygen delivery becomes apparent through reduced performance, faster fatigue, and prolonged recovery.
For athletes and health-conscious individuals, MCH abnormalities can be the first quantitative signal of iron deficiency or B12/folate insufficiency – often appearing before hemoglobin falls below the normal range. Catching a trending decline in MCH and investigating the cause (iron stores, B12, folate) allows correction before performance is significantly impacted and before the more visible and serious consequences of anemia develop.
Normal vs. Optimal MCH Levels
Standard Reference Ranges: Most laboratories report MCH as normal between 27 and 33 picograms (pg) per cell, though some labs use ranges of 26-34 pg. These ranges reflect the normal distribution of hemoglobin content in healthy adult red blood cells. MCH below 27 pg indicates hypochromic red blood cells (cells with less hemoglobin than normal). MCH above 33 pg indicates hyperchromic cells (cells with more hemoglobin than normal, usually because they are larger).
The Problem With “Normal”: Like MCV, MCH changes relatively late in the course of nutritional deficiencies. Iron deficiency progresses through stages of storage depletion, then transport impairment, then reduced hemoglobin synthesis – with MCH falling in the later stages. An MCH trending downward from 31 to 28 pg over two years warrants investigation of iron status even though both values are within the reference range. Similarly, an MCH trending upward toward 33+ pg warrants checking B12 and folate even if it remains technically normal.
Optimal MCH for Performance: An MCH of 29-32 pg alongside normal MCV, hemoglobin, and ferritin represents well-optimized red blood cell production. Athletes consuming adequate iron, B12, and folate with appropriate training loads typically maintain MCH in this range. Any MCH below 28 pg with concurrent low MCV strongly suggests iron deficiency and warrants ferritin and iron studies. Any MCH above 33 pg with high MCV warrants B12 and folate testing.
What Causes Low MCH (Hypochromic Cells)?
Iron deficiency is by far the most common cause of low MCH. When iron stores are depleted, the bone marrow cannot produce normal amounts of hemoglobin, resulting in small, pale (hypochromic) red blood cells with low MCH. This is the classic iron-deficiency anemia pattern – low MCV, low MCH, low MCHC, and low hemoglobin – though MCH may remain near-normal during early iron deficiency before hemoglobin synthesis is significantly impaired. Thalassemia trait (alpha or beta) also produces low MCH through impaired hemoglobin chain production rather than iron deficiency – distinguishing these requires checking ferritin (normal in thalassemia, low in iron deficiency). Anemia of chronic disease from inflammatory conditions, infections, autoimmune disease, and malignancy can reduce hemoglobin production and lower MCH. Lead poisoning impairs heme synthesis and reduces MCH. Sideroblastic anemias – from alcohol, medications, or rarely genetic causes – impair iron utilization for hemoglobin synthesis despite normal or elevated iron stores.
What Causes High MCH?
High MCH almost always accompanies high MCV (macrocytosis) – larger cells contain more hemoglobin. The causes of high MCH therefore mirror the causes of macrocytosis: vitamin B12 deficiency (impairs DNA synthesis, causes large immature red blood cells), folate deficiency (same mechanism), alcohol use (direct toxicity to bone marrow and impaired folate metabolism), hypothyroidism (slows cell production and maturation), and liver disease (alters red blood cell membrane composition). High MCH in isolation without elevated MCV is rare and usually artifactual. The underlying cause of any MCH elevation should be investigated because B12 deficiency in particular has neurological consequences beyond anemia that require treatment regardless of symptom severity.
Frequently Asked Questions
What is the difference between MCH and MCHC?
MCH measures the absolute amount of hemoglobin per cell (mass, in picograms). MCHC measures the concentration of hemoglobin within the cell – hemoglobin as a percentage of cell volume (g/dL). MCH changes with both cell size and hemoglobin content changes. MCHC specifically reflects hemoglobin packing density independent of cell size, making it the most specific indicator of true iron deficiency when consistently below 32 g/dL. Together, MCH and MCHC provide complementary perspectives on red blood cell hemoglobin content.
Can I have iron deficiency with normal MCH?
Yes. Early iron deficiency primarily depletes iron stores (ferritin) before affecting red blood cell production. MCH falls progressively with worsening deficiency – but during the early stages of iron-deficient erythropoiesis, MCH may remain in the normal range while ferritin is already very low and performance is affected. Ferritin is the most sensitive early biomarker for iron deficiency – not MCH. By the time MCH falls clearly below 27 pg, iron deficiency is typically established and ferritin is very low.
How long does it take for MCH to normalize after iron treatment?
Red blood cells live approximately 90-120 days. After starting effective iron treatment, new red blood cells with normal MCH begin entering circulation within a week, but the full blood population takes 2-3 months to turn over. Hemoglobin typically rises measurably within 2-4 weeks of treatment. MCH and MCV normalization follows over 2-3 months as the population of hypochromic microcytic cells is replaced. Iron stores (ferritin) take longer to replete – usually 3-6 months of supplementation to fully restore – and treatment should continue until ferritin is in the optimal range, not just until hemoglobin normalizes.
Are women more likely to have low MCH than men?
Yes. Premenopausal women lose iron through menstruation and face higher iron demands during pregnancy – making iron deficiency significantly more common in women than men. Iron deficiency affects an estimated 20-30% of premenopausal women in developed countries, and up to 50% in some populations. Athletic women face additional iron losses through sweat, foot-strike hemolysis (in runners), and increased demands from high training volumes. Regular comprehensive blood panels including ferritin, MCH, and MCHC are especially important for women of reproductive age who are physically active.
Testing MCH With ApexBlood
ApexBlood’s comprehensive panel includes the full red blood cell index – MCH, MCV, MCHC, hemoglobin, red blood cell count, ferritin, and iron studies – giving you the complete picture for red blood cell health assessment. Our physicians interpret these values in the context of your diet, training, symptoms, and full metabolic panel to identify what is driving any MCH abnormality and provide targeted treatment guidance.
Get comprehensive testing for $189
The Bottom Line on MCH
MCH is the per-cell hemoglobin metric that connects red blood cell size and overall hemoglobin capacity to the underlying nutritional or medical driver. Low MCH alongside low MCV and low ferritin is the hallmark of iron deficiency – the most common nutritional deficiency affecting performance. High MCH alongside high MCV points to B12 or folate deficiency, alcohol, or thyroid dysfunction. Monitoring MCH as part of a complete blood count and iron studies panel allows early identification of nutritional gaps before they progress to frank anemia and significant performance impact. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. MCH and red blood cell indices require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.