
MCHC – mean corpuscular hemoglobin concentration – is the most specific of the three red blood cell indices for detecting true iron deficiency and diagnosing certain rare but serious blood disorders. While MCV measures cell size and MCH measures total hemoglobin per cell, MCHC cuts through the size variable and measures hemoglobin density – how concentrated hemoglobin is within the cell regardless of the cell’s volume. A cell can be small but densely packed (hereditary spherocytosis), normal-sized but pale (iron deficiency), or large but appropriately filled (B12 deficiency). MCHC reveals this packing density directly, making it a precision instrument in the red blood cell index toolkit for anyone trying to understand exactly what is driving an abnormality in their CBC.
What Is MCHC?
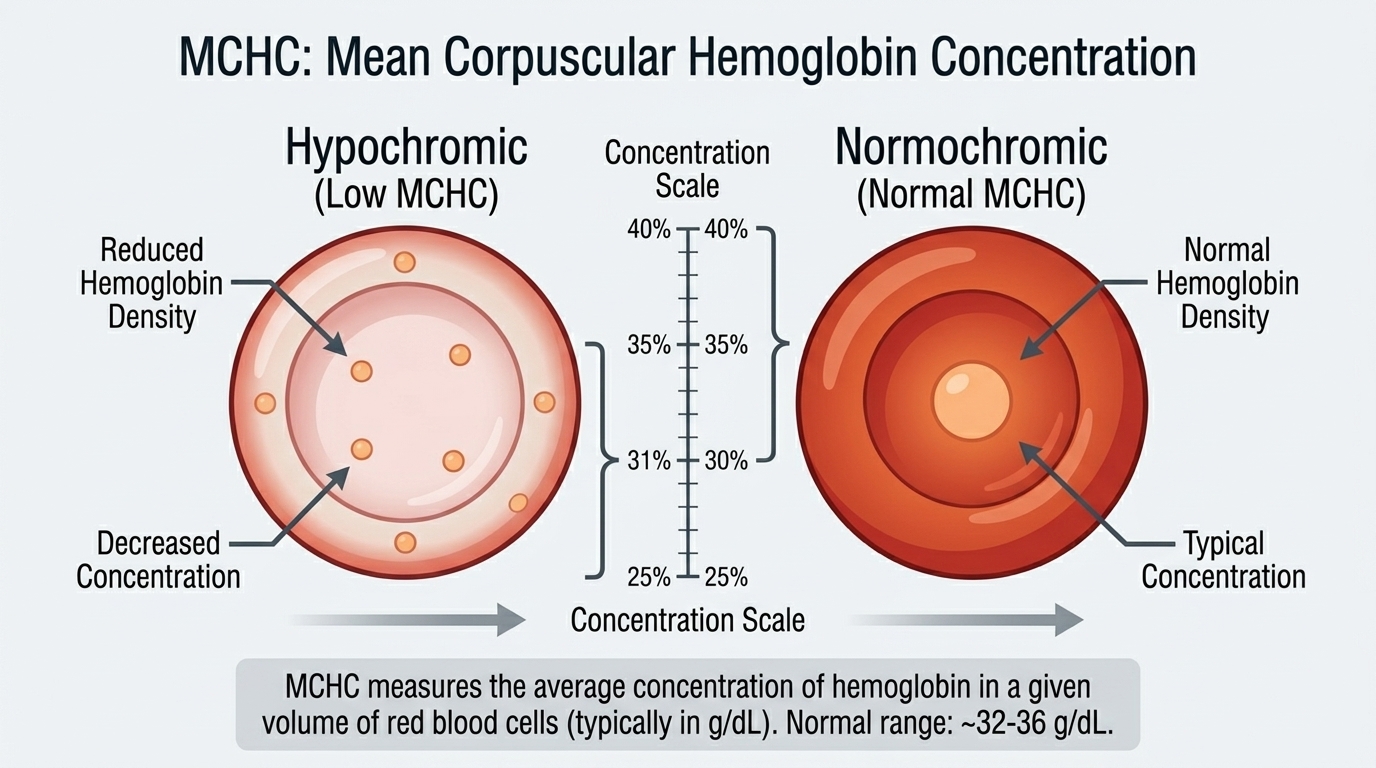
MCHC stands for mean corpuscular hemoglobin concentration. It measures the average concentration of hemoglobin in a given volume of red blood cells, expressed in grams per deciliter (g/dL). It is calculated as hemoglobin (g/dL) divided by hematocrit (the fraction of blood volume occupied by red blood cells), multiplied by 100. The result represents how much of the available space inside the average red blood cell is occupied by hemoglobin.
Hemoglobin concentration within a cell is constrained by biology – cells cannot pack hemoglobin beyond a certain saturation point without affecting their deformability and function. This biological ceiling means that truly high MCHC (hyperchromia) is uncommon and when present is almost always significant – hereditary spherocytosis and certain hemolytic anemias being the classic causes. Low MCHC (hypochromia) is more common and reflects inadequate hemoglobin synthesis relative to cell volume, most often from iron deficiency.
Why MCHC Matters for Red Blood Cell Function
Red blood cells depend on optimal hemoglobin concentration to function effectively. MCHC that is too low means cells are pale and hemoglobin-depleted relative to their size – unable to carry as much oxygen per cell as normal. MCHC that is too high can signal a structural abnormality in the red blood cell membrane (as in spherocytosis) that causes premature cell destruction and hemolytic anemia. For performance-focused individuals, MCHC fits into the broader picture of red blood cell optimization – alongside ferritin, iron, B12, folate, and total hemoglobin – to identify the specific nature of any suboptimal oxygen-carrying capacity.
MCHC is particularly valuable as a quality control marker and as the most specific indicator of iron-deficiency erythropoiesis (iron-deficient red blood cell production). When MCHC falls clearly below 32 g/dL in an adult, this almost always means iron deficiency is causing hypochromic red blood cells regardless of what MCV and MCH show. This specificity makes MCHC an important confirmatory marker when other red blood cell indices are equivocal.
Normal vs. Optimal MCHC Levels
Standard Reference Ranges: MCHC is normally reported between 31.5 and 36 g/dL, with some laboratories using 32-36 g/dL. Red blood cells are biologically constrained in how much hemoglobin they can concentrate, so the upper end of this range represents near-maximal hemoglobin packing in normal cells. MCHC above 36 g/dL is unusual and warrants investigation for hereditary spherocytosis, certain hemolytic anemias, or laboratory artifact (cold agglutinins, lipemia, very high white cell counts can falsely elevate MCHC).
The Problem With “Normal”: A normal MCHC does not rule out iron deficiency – early iron deficiency depletes ferritin and progressively impairs hemoglobin synthesis, but MCHC may remain in the low-normal range (32-33 g/dL) while iron stores are already substantially depleted. MCHC trends toward the lower end of normal during iron depletion before falling below the reference range in established iron-deficiency anemia. As with MCV and MCH, serial monitoring with attention to trend matters as much as any single value.
Optimal MCHC for Performance: An MCHC of 33-35 g/dL alongside normal MCV, MCH, hemoglobin, and ferritin indicates healthy, well-loaded red blood cells with optimal oxygen-carrying density. MCHC consistently at the low end of normal (31-32 g/dL) alongside any decline in MCV or MCH warrants checking ferritin and iron studies for early iron deficiency.
What Causes Low MCHC (Hypochromia)?
Iron deficiency is the predominant cause of low MCHC. Without adequate iron, heme synthesis is impaired, hemoglobin production falls, and red blood cells emerge from the bone marrow with insufficient hemoglobin relative to their volume – appearing pale on blood smear and showing low MCHC on CBC. The low MCHC pattern in iron deficiency typically accompanies low MCV (microcytic) and low MCH (hypochromic), though MCHC can fall before MCV becomes clearly microcytic. Thalassemia produces microcytic, hypochromic cells with low MCHC similar to iron deficiency, but ferritin is normal or elevated. Sideroblastic anemia (from lead, alcohol, certain medications, or rarely genetic causes) impairs heme synthesis despite normal iron stores. Anemia of chronic disease from inflammatory conditions occasionally produces low-normal MCHC.
What Causes High MCHC?
Hereditary spherocytosis is the classic cause of true MCHC elevation – this genetic red blood cell membrane disorder causes cells to lose their biconcave disc shape and become spherical, reducing surface area relative to volume and increasing hemoglobin concentration. Spherocytes are rigid and fragile, prone to destruction in the spleen (hemolytic anemia). MCHC above 36 g/dL on multiple measurements is one of the screening findings that prompts evaluation for hereditary spherocytosis. Sickle cell disease can produce elevated MCHC in sickled cells. Cold agglutinins (antibodies that cause red blood cells to clump at low temperatures) cause laboratory artifact that falsely elevates MCHC. Severe lipemia (high fat content in blood) can interfere with the spectrophotometric measurement used to calculate hemoglobin and produce falsely elevated MCHC.
Frequently Asked Questions
Why is MCHC considered more specific than MCH for iron deficiency?
MCH (absolute hemoglobin per cell) changes with both cell size and hemoglobin content – you can have low MCH because cells are small (even if hemoglobin-packed) or because they are hypochromic. MCHC corrects for cell size by expressing hemoglobin relative to cell volume (hematocrit), so it specifically reflects hemoglobin packing density regardless of whether cells are big or small. This makes MCHC below 32 g/dL a more specific indicator that cells are genuinely hemoglobin-depleted – which in adults is almost always from iron deficiency when other causes are excluded.
Can MCHC be high if I have B12 deficiency?
In B12 or folate deficiency, red blood cells are larger than normal (macrocytic, high MCV) but typically contain appropriate hemoglobin for their size. MCHC is usually normal in B12/folate deficiency because the cells, while oversized, are not abnormally concentrated. The high MCH seen with B12 deficiency reflects the larger cell size containing more total hemoglobin, not higher hemoglobin concentration. MCHC stays normal. This is a key distinguishing feature – low MCHC points to iron deficiency/hypochromia; normal MCHC with high MCV/MCH points to macrocytic causes like B12 or folate deficiency.
What is hereditary spherocytosis and how does MCHC help diagnose it?
Hereditary spherocytosis is an inherited disorder of red blood cell membrane proteins that causes cells to lose their flexible biconcave disc shape and become rigid spheres. These spherocytes are destroyed in the spleen faster than normal, causing chronic hemolytic anemia of variable severity. Key features include anemia, elevated bilirubin and jaundice (from increased red blood cell breakdown), splenomegaly, and a higher-than-normal MCHC (often 35-38 g/dL) because the spherical shape increases hemoglobin concentration relative to surface area. MCHC above 36 g/dL on repeat testing is one of the screening criteria that prompts osmotic fragility testing, eosin-5-maleimide (EMA) flow cytometry, or genetic testing to confirm spherocytosis.
Do I need to worry about a slightly low MCHC if my hemoglobin is normal?
A mildly low MCHC (31-32 g/dL) with normal hemoglobin suggests early iron-deficient erythropoiesis – red blood cells are being produced with slightly less hemoglobin than optimal, but the total hemoglobin in the blood remains adequate because the body is compensating with red blood cell production. This pattern warrants checking ferritin. If ferritin is below 30-50 ng/mL, iron deficiency is almost certainly the cause and supplementation is appropriate. Addressing iron deficiency at this stage prevents progression to frank anemia and optimizes red blood cell quality before performance is significantly impacted.
Testing MCHC With ApexBlood
MCHC is part of ApexBlood’s comprehensive CBC panel alongside MCV, MCH, hemoglobin, ferritin, and iron studies – providing the complete red blood cell index assessment needed to diagnose the specific cause of any hematologic abnormality. Our physicians interpret all indices together rather than flagging individual values in isolation, giving you actionable insight into what your red blood cells reveal about your nutritional status and overall health.
Get comprehensive testing for $189
The Bottom Line on MCHC
MCHC is the hemoglobin concentration index – measuring how densely packed your red blood cells are with oxygen-carrying hemoglobin relative to their volume. Low MCHC is the most specific indicator of iron-deficient erythropoiesis among the red blood cell indices. High MCHC raises the question of hereditary spherocytosis and warrants further evaluation. Normal MCHC with other abnormal indices guides the diagnostic workup in a different direction. No single CBC value tells the complete story – MCHC is most powerful when interpreted as part of the full red blood cell picture alongside MCV, MCH, ferritin, and iron studies. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. MCHC and red blood cell indices require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.