
Monocytes: What This Overlooked Immune Marker Reveals About Inflammation, Infection, and Longevity
Your doctor reviews your complete blood count, sees monocytes at 11%, and says nothing. It’s “within range.” You move on.
But elevated monocytes are your immune system telling you something is wrong – chronic inflammation smoldering beneath the surface, an infection your body is quietly fighting, or early metabolic dysfunction that hasn’t shown up anywhere else yet. Monocytes are frontline soldiers in your immune defense, and when their numbers are persistently elevated or suppressed, it’s a signal worth understanding.
Most people have never heard of monocytes. They’re not the headline biomarker that cholesterol or testosterone are. But for anyone serious about optimizing their biology, monocytes provide a window into immune function, systemic inflammation, and long-term health that most standard blood panels barely acknowledge.
High performers don’t ignore immune markers just because they’re asymptomatic. They measure, they understand, they optimize.
What Are Monocytes?
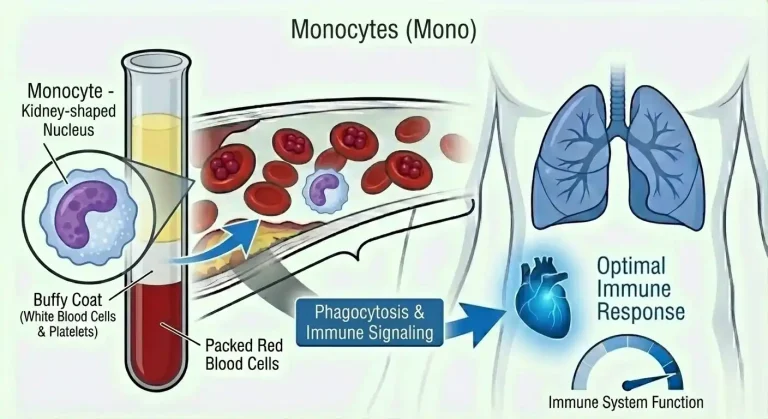
Monocytes are a type of white blood cell – specifically, the largest of all circulating white blood cells. They’re produced in the bone marrow and make up roughly 2-8% of total white blood cells in healthy adults. They circulate in the bloodstream for 1-3 days before migrating into tissues, where they mature into macrophages or dendritic cells – two of the most powerful immune responders in the body.
As macrophages, they become your tissue’s cleanup crew and command center. They engulf and destroy pathogens, dead cells, and cellular debris (a process called phagocytosis). They present antigens to other immune cells, essentially flagging threats and coordinating the adaptive immune response. They secrete cytokines – chemical signals that amplify or dampen inflammation depending on what the situation demands.
Monocytes are divided into three subpopulations based on surface protein expression. Classical monocytes make up the majority (roughly 85-90%) and are primarily involved in surveillance and pathogen clearance. Intermediate monocytes are fewer in number but highly inflammatory – they’re elevated in cardiovascular disease, sepsis, and chronic inflammatory conditions. Non-classical monocytes patrol blood vessel walls and monitor for damage, playing a role in atherosclerosis and vascular inflammation.
Standard blood panels don’t differentiate between subtypes. They report a single monocyte count or percentage. But understanding that monocytes aren’t a monolithic population is important context for interpreting elevated levels – the type of monocyte driving the elevation matters considerably.
Why Monocytes Matter for Performance and Health
Monocytes occupy a central position in the connection between immune function, inflammation, and virtually every chronic disease that degrades performance and longevity.
Immune defense is the obvious role. When a pathogen enters your body, monocytes are among the first responders. They move to the site of infection, engulf bacteria and viruses, and help coordinate the broader immune response. If your monocyte count is low, your first-line immune defense is compromised. You’re slower to respond to infections, slower to clear them, and more vulnerable to opportunistic pathogens.
Inflammation regulation is where monocytes become particularly relevant to high performers. Macrophages derived from monocytes are key drivers of both acute and chronic inflammation. When they’re appropriately activated and then resolved, inflammation serves its purpose – clearing damage, fighting infection, facilitating repair. When they’re chronically activated (from persistent infection, metabolic dysfunction, visceral fat, poor diet, or environmental stressors), they produce a sustained low-grade inflammatory state that damages tissues, accelerates biological aging, and impairs virtually every system in the body.
Elevated monocytes in the absence of obvious infection are often the immune system’s fingerprint of chronic inflammation. This matters because chronic low-grade inflammation is implicated in cardiovascular disease, insulin resistance, cognitive decline, depression, cancer progression, and accelerated cellular aging. Monocytes don’t cause these conditions directly – but persistently elevated monocytes are a signal that the inflammatory environment driving them is active.
Cardiovascular risk is directly connected to monocyte function. Monocytes are central players in atherosclerosis – the process by which plaque accumulates in arterial walls. When LDL cholesterol is oxidized and deposited in arterial walls, monocytes migrate into the vessel wall, differentiate into macrophages, and engulf the oxidized LDL. These lipid-laden macrophages become foam cells, and their accumulation forms the fatty streaks that eventually develop into atherosclerotic plaques. Elevated intermediate monocytes specifically are associated with increased cardiovascular risk independent of traditional lipid markers.
Metabolic health is closely linked to monocyte activation. Visceral fat is metabolically active tissue that continuously secretes inflammatory signals, including those that recruit and activate monocytes. Insulin resistance drives chronic inflammation through multiple mechanisms that involve monocyte activation. Elevated monocytes in otherwise healthy, asymptomatic individuals often reflect underlying metabolic dysfunction before it’s apparent in glucose, insulin, or HbA1c levels.
Longevity and biological aging are influenced by monocyte polarization. Research on aging consistently shows that chronic low-grade inflammation – sometimes called “inflammaging” – is one of the primary biological mechanisms driving accelerated aging and age-related disease. Monocytes and their tissue derivatives are key contributors to inflammaging. High performers focused on longevity need to understand that keeping systemic inflammation in check, including monitoring immune markers like monocytes, is core to optimizing the biological aging process.
Normal vs. Optimal Monocyte Levels
Standard reference ranges for monocytes on a complete blood count (CBC) are typically:
Percentage of white blood cells: 2-8%
Absolute monocyte count: 0.2-0.9 x 10^9/L (or 200-900 cells per microliter)
These ranges are, as with most standard reference intervals, based on population averages that include people with chronic illness, poor metabolic health, and persistent low-grade infection.
The problem with “normal”: Someone with monocytes consistently at 8% is technically within range. But if that person is in good health with no acute infection or inflammatory condition, sitting at the top of the reference range likely reflects elevated baseline inflammation that warrants investigation – not reassurance.
Optimal monocyte levels for performance and longevity:
Percentage: 2-6% of total white blood cells
Absolute count: 200-600 cells per microliter
Healthy, metabolically fit individuals with low systemic inflammation and good immune function typically show monocytes in the lower half of the reference range. Consistently elevated monocytes – particularly in the 8-10%+ range without a clear acute cause – warrant investigation rather than dismissal.
Context matters here. A single elevated monocyte reading means very little on its own. Monocytes fluctuate in response to stress, exercise, sleep deprivation, subclinical infections, and dozens of other variables. What matters is the trend over time, the level of elevation, and whether it’s accompanied by other inflammatory markers that corroborate chronic immune activation.
What Causes Elevated Monocytes?
Understanding what drives elevated monocytes is essential for interpreting the signal correctly.
Acute infections are the most common cause of temporarily elevated monocytes. Bacterial infections, viral infections (particularly Epstein-Barr virus, cytomegalovirus, and HIV), fungal infections, and parasitic infections all stimulate monocyte production. This is an appropriate, functional immune response. Monocytes should be elevated when your body is fighting an infection. The key question is whether they return to baseline after the infection resolves.
Chronic infections produce persistently elevated monocytes that can be subtle. Low-grade chronic infections including H. pylori, Lyme disease, tuberculosis, and certain viral infections maintain ongoing immune activation. These are often missed on standard workups because acute symptoms are absent, but monocyte elevation persists as evidence that the immune system is still engaged.
Chronic inflammatory conditions are a major driver of persistently elevated monocytes. Autoimmune diseases (rheumatoid arthritis, lupus, inflammatory bowel disease, multiple sclerosis) involve ongoing immune activation that keeps monocyte counts elevated. Inflammatory bowel conditions including Crohn’s disease and ulcerative colitis show consistently elevated monocytes during active disease. Even asymptomatic autoimmune conditions can produce elevated monocyte counts before other clinical signs appear.
Metabolic dysfunction and obesity are increasingly recognized as major contributors to monocyte elevation. Visceral adipose tissue functions as an endocrine organ that secretes inflammatory cytokines (including TNF-alpha, IL-6, and MCP-1, which specifically recruits monocytes). Insulin resistance and elevated blood glucose create an inflammatory environment that activates monocytes chronically. This is why elevated monocytes in overweight or obese individuals often reflect metabolic inflammation rather than infection.
Cardiovascular disease is both a cause and a consequence of elevated monocyte activity. Atherosclerotic plaques contain activated macrophages derived from monocytes. The inflammatory process driving plaque formation keeps monocytes elevated, and their continued activity accelerates plaque progression.
Recovery from acute illness or injury temporarily elevates monocytes. Monocytes are critical for tissue repair – they clear debris, produce growth factors, and coordinate regenerative processes. Elevated monocytes following surgery, trauma, or acute illness reflect this repair process.
Certain medications can elevate monocytes, including corticosteroids (particularly during taper), granulocyte colony-stimulating factors used in cancer treatment, and certain immunomodulatory drugs.
Hematologic conditions in rare cases cause dramatically elevated monocytes. Chronic myelomonocytic leukemia (CMML) is characterized by persistently very high monocyte counts (above 1,000 cells/microliter) and requires hematologic evaluation. Monocytic leukemia and other bone marrow disorders can present with marked monocytosis. While these are uncommon, very high or rapidly rising monocyte counts warrant medical evaluation.
Stress and poor sleep contribute to monocyte elevation through cortisol and catecholamine pathways. Chronic psychological stress activates the sympathetic nervous system and HPA axis, which upregulates monocyte production and inflammatory activation. Sleep deprivation, even short term, produces measurable increases in monocyte counts and inflammatory markers.
What Causes Low Monocytes?
Monocytopenia – abnormally low monocyte counts below 200 cells per microliter – is less common but clinically significant.
Bone marrow suppression is the most common cause. Chemotherapy and radiation therapy damage bone marrow and reduce production of all white blood cells including monocytes. Aplastic anemia, a condition where bone marrow fails to produce adequate blood cells, causes monocytopenia along with reductions in other cell lines.
Severe or prolonged infection can paradoxically deplete monocytes. Overwhelming sepsis or advanced HIV infection can exhaust monocyte reserves faster than the bone marrow can replenish them.
Autoimmune conditions in some cases produce autoantibodies against monocytes, reducing circulating counts.
Hairy cell leukemia is a rare blood cancer specifically associated with monocytopenia – monocyte counts near zero are actually a diagnostic clue for this condition.
Corticosteroid therapy initially elevates monocytes but chronic high-dose corticosteroid use can eventually suppress monocyte production.
Persistently low monocytes indicate compromised immune surveillance capacity. People with monocytopenia have impaired ability to respond to infections – particularly fungal, parasitic, and intracellular bacterial infections – and slower clearance of cellular debris and damaged tissue.
How to Optimize Monocyte Levels
If monocytes are elevated without an acute infectious cause, the focus should be on reducing the underlying chronic inflammation driving the elevation.
Address metabolic health first. If visceral fat, insulin resistance, or elevated blood glucose is present, this is likely the primary driver of chronically elevated monocytes. Weight loss – particularly visceral fat reduction – produces measurable decreases in systemic inflammation and monocyte counts. Reducing refined carbohydrates and sugar, improving insulin sensitivity through diet and exercise, and achieving and maintaining healthy body composition are foundational interventions.
Optimize sleep. Sleep is when the immune system resets and inflammatory cytokines clear. Chronic sleep deprivation maintains elevated monocyte counts and inflammatory markers. Consistent 7-9 hours of quality sleep is one of the most impactful interventions for reducing systemic inflammation.
Reduce chronic psychological stress. Chronic stress activates inflammatory pathways and upregulates monocyte production. Stress management isn’t a soft lifestyle recommendation – it’s a direct intervention for immune dysregulation. Exercise, mindfulness, adequate recovery, and reducing unnecessary stressors all reduce chronic stress-driven inflammation.
Exercise strategically. Regular moderate-intensity exercise consistently reduces systemic inflammation and optimizes immune function. However, excessive training without adequate recovery can temporarily elevate monocytes and other inflammatory markers. High performers benefit from structured periodization and intentional recovery rather than constant high-intensity output.
Optimize diet for anti-inflammatory intake. An anti-inflammatory dietary pattern – emphasizing whole foods, vegetables, berries, fatty fish rich in omega-3s, olive oil, and minimizing processed foods, refined carbohydrates, and industrial seed oils – directly reduces the inflammatory stimulus for monocyte activation. Omega-3 fatty acids from fish or quality supplements have well-documented anti-inflammatory effects, partly through their influence on monocyte and macrophage polarization.
Investigate and treat chronic infections. If monocytes are persistently elevated without an obvious metabolic cause, consider screening for chronic infections including H. pylori, Lyme disease, CMV, EBV, and other subclinical infectious drivers. Treating an underlying chronic infection often normalizes monocyte counts.
Monitor and manage inflammatory conditions. If you have an autoimmune or inflammatory condition, optimizing its management – with your physician’s guidance – reduces the immune activation that keeps monocytes elevated.
Monocytes and Other Health Markers
Monocytes don’t tell their full story in isolation. They’re most informative alongside other immune and inflammatory markers.
hs-CRP (high-sensitivity C-reactive protein) is a direct measure of systemic inflammation. Elevated hs-CRP and elevated monocytes together provide strong corroborating evidence of chronic inflammatory activation. Optimal hs-CRP is below 1.0 mg/L, ideally below 0.5 mg/L.
Complete blood count with differential provides the full white blood cell picture. Neutrophils, lymphocytes, eosinophils, and basophils alongside monocytes tell a more complete immune story. Elevated neutrophils with elevated monocytes suggests bacterial infection or significant stress. Elevated lymphocytes suggest viral activity. Elevated eosinophils alongside monocytes can indicate parasitic infection or allergic inflammation.
Ferritin is both an iron storage marker and an acute phase protein – it rises with inflammation. Elevated ferritin in the setting of elevated monocytes (without iron deficiency) can indicate chronic inflammatory or infectious disease.
Metabolic markers including fasting insulin, glucose, and HbA1c help determine whether metabolic dysfunction is driving monocyte elevation. The monocyte-to-HDL ratio is an emerging marker for cardiovascular risk that reflects the balance between atherogenic immune activation (monocytes) and protective reverse cholesterol transport (HDL).
Homocysteine is an independent cardiovascular risk factor that often tracks with systemic inflammation and immune activation.
Vitamin D deficiency is associated with immune dysregulation and elevated inflammatory markers. Optimal vitamin D (50-70 ng/mL) supports appropriate immune function and modulates monocyte activity.
Monocytes and Longevity Treatments
For individuals focused on longevity and biological optimization, the connection between chronic inflammation, immune aging, and monocyte biology is increasingly relevant.
Chronic low-grade inflammation driven by persistently activated monocytes and macrophages is a central mechanism of inflammaging – the progressive inflammatory state that accompanies biological aging and accelerates age-related disease. Strategies that reduce chronic monocyte activation directly address one of the primary biological drivers of accelerated aging.
Metformin, in addition to its metabolic benefits, has demonstrated anti-inflammatory effects including modulation of monocyte and macrophage activation. In individuals with insulin resistance or metabolic dysfunction driving inflammatory monocyte elevation, metformin addresses both the metabolic root cause and the inflammatory downstream effects.
NAD+ plays a role in cellular energy production and has been studied for its influence on macrophage function and inflammatory signaling. As NAD+ levels decline with age – a consistent finding in aging biology – immune cell function, including monocyte and macrophage activity, is affected.
These interventions aren’t a replacement for addressing the lifestyle drivers of chronic inflammation. They work best as part of a comprehensive approach that addresses root causes rather than just managing downstream markers.
Frequently Asked Questions
What is a normal monocyte count?
Standard reference ranges show 2-8% of white blood cells, or 200-900 cells per microliter in absolute terms. However, for people in good metabolic health without chronic inflammation or infection, optimal monocyte levels are typically in the lower half of this range – roughly 2-6% or 200-600 cells per microliter. Consistently sitting at the top of the reference range without an obvious cause warrants investigation.
What does it mean if my monocytes are high?
It depends on context. In the setting of recent infection, illness, or physical stress, temporarily elevated monocytes are a normal immune response. Persistently elevated monocytes in an otherwise asymptomatic person more often reflect chronic low-grade inflammation, subclinical infection, metabolic dysfunction, or an underlying inflammatory condition. A single elevated reading is less meaningful than a pattern across multiple measurements.
Can stress elevate monocytes?
Yes. Chronic psychological stress activates the HPA axis and sympathetic nervous system, both of which upregulate monocyte production and inflammatory activation. People with high baseline stress levels often show elevated monocytes and other inflammatory markers even without infection or obvious medical conditions.
Are monocytes related to cardiovascular risk?
Directly, yes. Monocytes – specifically intermediate monocytes – are central to the atherosclerotic process. They migrate into arterial walls in response to oxidized LDL, differentiate into macrophages, and become foam cells that contribute to plaque formation. Elevated circulating monocytes are independently associated with cardiovascular risk beyond traditional markers like total cholesterol.
How often should monocytes be checked?
For most people, monocytes are included in a standard complete blood count (CBC), which is part of comprehensive blood testing. Annual testing is appropriate for healthy adults. If monocytes are consistently elevated or if you’re actively working to reduce chronic inflammation, testing every 3-6 months allows you to track your response to interventions.
Can monocytes be too low?
Yes. Monocytopenia (below 200 cells per microliter) indicates compromised immune surveillance and is associated with impaired ability to fight infections – particularly fungal, parasitic, and intracellular bacterial infections. Very low monocytes require medical evaluation to identify the cause, which may include bone marrow disorders, severe infection, or medication effects.
Do elevated monocytes always mean infection?
No. While infection is a common cause, chronically elevated monocytes in the absence of acute infection more commonly reflect metabolic inflammation, chronic low-grade infection, autoimmune activity, or cardiovascular disease processes. Context from other markers and clinical history is essential for interpretation.
What’s the difference between monocytes and macrophages?
Monocytes are immature immune cells that circulate in the bloodstream. When they migrate into tissues, they mature into macrophages – tissue-resident immune cells that perform phagocytosis, antigen presentation, and cytokine secretion. Macrophages are the activated, tissue-based form of monocytes. When you see elevated circulating monocytes, it often reflects increased demand for macrophage activity in tissues.
Testing Monocytes With ApexBlood
Monocytes are included in the complete blood count (CBC) with differential that’s part of ApexBlood’s comprehensive 100+ biomarker blood panel. But monocytes tell their most useful story alongside the other markers that reveal what’s driving their elevation – hs-CRP, ferritin, metabolic markers, and the full immune picture that context requires.
Understanding whether elevated monocytes reflect metabolic dysfunction, chronic inflammation, subclinical infection, or something else entirely requires looking at the complete biological picture – not a single number in isolation. That’s why comprehensive testing exists. You can’t understand one marker without seeing what surrounds it.
Most physicians check a CBC reactively when you’re sick. High performers test proactively to establish baselines, track trends, and catch immune dysregulation and chronic inflammation before they translate into disease.
Get comprehensive testing – $189
The Bottom Line on Monocytes
Monocytes are your immune system’s frontline responders and the link between chronic inflammation, metabolic health, cardiovascular disease, and biological aging. They’re rarely discussed outside clinical medicine, but for anyone serious about optimizing their biology, they’re worth understanding and monitoring.
Optimal monocytes are 2-6% of white blood cells (200-600 cells per microliter). Standard “normal” extends to 8% and captures people with smoldering chronic inflammation. Persistently elevated monocytes without an acute infectious cause are a signal – chronic metabolic inflammation, subclinical infection, autoimmune activity, or cardiovascular disease processes – not a finding to dismiss.
Low monocytes indicate compromised immune defense that leaves you slower to respond to infection and impaired in tissue repair.
Optimizing monocyte levels isn’t about targeting the number directly – it’s about addressing the root causes of chronic immune activation: metabolic health, sleep, stress, diet, chronic infection, and systemic inflammation. When those are addressed, monocyte counts normalize as a reflection of improved biological health.
High performers don’t wait for clinical disease to appear before they address immune dysregulation. They measure, they understand the signal, and they act on it.
You can’t optimize what you don’t measure. Stop accepting “within normal range” when optimal immune function and minimal chronic inflammation are achievable.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Monocyte levels and immune health require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.