
Potassium is the primary electrolyte inside your cells, and it is essential for functions most people take completely for granted: every heartbeat, every muscle contraction, every nerve impulse, and your kidneys’ ability to regulate blood pressure all depend on potassium. Yet potassium rarely gets the attention it deserves in mainstream health discussions – most people know vaguely that bananas have potassium but have little understanding of what their potassium level actually means for their performance, cardiac health, and longevity. Your doctor may check your potassium on a routine panel, note that it falls in the “normal” range, and move on without discussion. But potassium, like most biomarkers, has a wide “normal” range that obscures meaningful differences in health and performance between the upper and lower ends of that range.
What Is Serum Potassium?
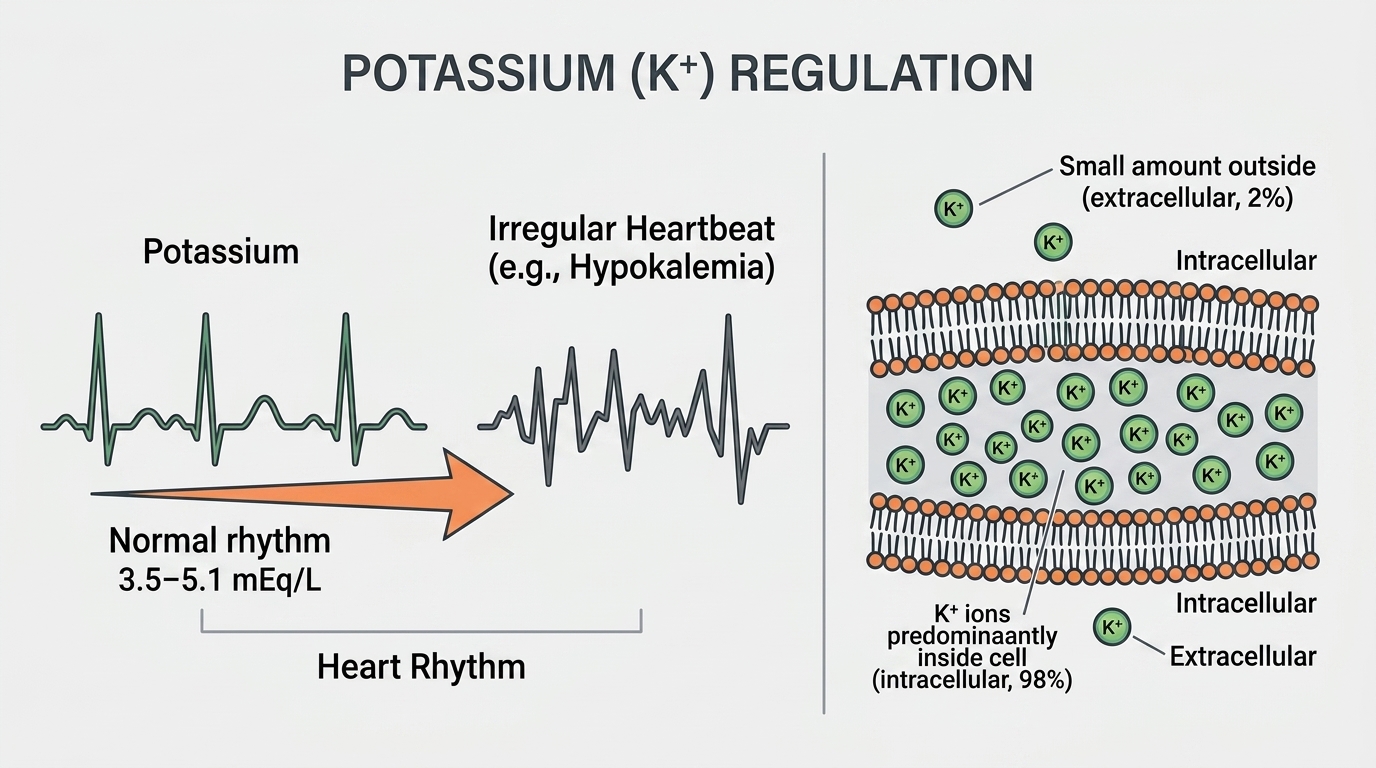
Serum potassium measures the concentration of potassium ions in your blood plasma. Potassium is the predominant intracellular cation – about 98% of your body’s potassium is inside cells, primarily in muscle cells. Only about 2% is in the bloodstream, which is what serum potassium measures. This distribution is actively maintained by the sodium-potassium ATPase pump – the molecular machine in every cell membrane that continuously moves potassium in and sodium out, creating the electrochemical gradients that make nerve and muscle function possible.
Because intracellular potassium is so much higher than extracellular potassium, small changes in serum potassium can reflect large shifts in the intracellular pool. Similarly, conditions that shift potassium between the inside and outside of cells – insulin, pH changes, catecholamines (adrenaline) – can rapidly alter serum potassium without changing total body potassium. This is why serum potassium must always be interpreted in clinical context rather than as an absolute indicator of total body potassium stores.
Why Potassium Matters for Performance and Longevity
Potassium’s most immediately critical role is in cardiac function. The resting membrane potential of cardiac muscle cells – the electrical state they must return to before firing the next heartbeat – depends on the potassium gradient across the cell membrane. When serum potassium deviates from the optimal range, this membrane potential is disrupted, producing abnormal cardiac rhythms. Both hypokalemia (low potassium) and hyperkalemia (high potassium) can cause dangerous arrhythmias, which is why potassium is one of the most closely monitored electrolytes in hospitalized patients and why diuretic prescriptions routinely include potassium monitoring.
Beyond cardiac rhythm, potassium is essential for skeletal muscle function and smooth muscle function including in blood vessels. Low potassium impairs muscle strength and endurance, causes cramping, and contributes to blood pressure elevation through reduced vascular smooth muscle relaxation. For athletes and high performers, potassium status directly affects training capacity, recovery time, and cardiovascular efficiency. The high prevalence of inadequate potassium intake in Western diets – the average American consumes roughly half the recommended intake – represents a genuine and commonly overlooked performance drag.
Normal vs. Optimal Potassium Levels
Standard Reference Ranges: Most laboratories report serum potassium as normal between 3.5 and 5.0 mEq/L (or mmol/L). Below 3.5 mEq/L is hypokalemia. Above 5.0 mEq/L is hyperkalemia. These boundaries are clinically important – outside these ranges, arrhythmia risk rises meaningfully, particularly at extremes (below 3.0 or above 6.0 mEq/L).
The Problem With “Normal”: Serum potassium at 3.6 mEq/L and 4.8 mEq/L are both “normal.” From a performance and cardiovascular health perspective, they are not equivalent. Research consistently shows that the optimal potassium range for minimizing cardiovascular risk and arrhythmia risk is 4.0-5.0 mEq/L – the upper half of the reference range. Potassium in the 3.5-4.0 mEq/L range is associated with higher rates of cardiac arrhythmia in people with underlying heart disease, and the cardiovascular benefit of higher potassium intake is well-documented across population studies.
Optimal Potassium for Performance: For most healthy adults, serum potassium between 4.0 and 4.8 mEq/L represents the sweet spot – adequate for cardiac stability, neuromuscular function, and blood pressure regulation. Low-normal potassium (3.5-3.9 mEq/L) alongside low dietary potassium intake suggests room for optimization through diet, and potentially supplementation in consultation with a physician. Values consistently above 5.0 mEq/L require investigation to rule out kidney dysfunction, medication effects, or sampling artifacts (hemolysis can falsely elevate potassium dramatically and is a common lab error).
What Causes Low Potassium (Hypokalemia)?
Inadequate dietary potassium is the most common underlying contributor, particularly in diets heavily dominated by processed foods that are low in potassium and high in sodium. But significant hypokalemia (below 3.5 mEq/L) usually has an additional driver: losses from the kidneys or gut. Diuretics – particularly thiazide and loop diuretics – are the most common clinical cause of hypokalemia because they force potassium excretion in the kidneys as a side effect of increasing urine output. Vomiting and diarrhea cause significant potassium losses through the gut. Excessive sweating during intense exercise or heat exposure can deplete potassium alongside sodium. Hypomagnesemia (low magnesium) causes renal potassium wasting and makes hypokalemia refractory to treatment – potassium cannot be fully replaced when magnesium is depleted. Certain medications including insulin, beta-agonists (like albuterol inhalers), and some antibiotics can shift potassium into cells, lowering serum levels. Primary hyperaldosteronism (an adrenal gland tumor or hyperplasia causing excess aldosterone) is an underdiagnosed cause of persistent hypokalemia and hypertension worth considering in resistant cases.
What Causes High Potassium (Hyperkalemia)?
Kidney disease is the most common cause of true hyperkalemia – the kidneys are the primary route for potassium excretion, and when kidney function is impaired, potassium accumulates. ACE inhibitors, ARBs (common blood pressure medications), potassium-sparing diuretics, and NSAIDs can all cause or worsen hyperkalemia, particularly in people with underlying kidney impairment. Adrenal insufficiency (Addison’s disease) causes hyperkalemia through aldosterone deficiency – without adequate aldosterone, the kidneys cannot excrete potassium efficiently. Type 4 renal tubular acidosis, common in diabetic kidney disease, impairs potassium excretion. Pseudohyperkalemia from red blood cell hemolysis during blood collection is very common – if potassium is unexpectedly high without symptoms, repeat the test. Excessive potassium supplementation without medical oversight in people with any kidney impairment can be dangerous.
How to Optimize Potassium Levels
For most people with low-normal or dietary potassium inadequacy, increasing food-based potassium is the most effective and safest approach. The best dietary sources of potassium include: avocados (975 mg per medium avocado), sweet potatoes (700+ mg per medium), white potatoes (940 mg per medium with skin), spinach and other leafy greens, salmon and other fatty fish, bananas (420 mg each), beans and lentils, and dairy products. The daily adequate intake for potassium is 2,600 mg for women and 3,400 mg for men – intake that most Americans fall short of. The sodium-to-potassium ratio in the diet matters as much as absolute potassium intake for cardiovascular outcomes – replacing processed foods (high sodium, low potassium) with whole foods (lower sodium, higher potassium) simultaneously moves both variables in the right direction. Potassium supplementation in otherwise healthy people with adequate kidney function is generally safe at modest doses (99-200 mg per tablet), but high-dose supplementation always warrants physician oversight given the cardiac risk of hyperkalemia.
Potassium and Blood Pressure
The relationship between potassium and blood pressure is one of the most robust in nutritional science. Potassium causes vasodilation by relaxing vascular smooth muscle, stimulates sodium excretion through the kidneys (reducing blood volume), and reduces the blood pressure-raising effect of sodium intake. Meta-analyses consistently show that increasing potassium intake reduces systolic blood pressure by 3-8 mmHg on average – an effect size comparable to modest sodium restriction and additive to it. Given that blood pressure control is one of the highest-leverage interventions for reducing cardiovascular disease, stroke, and kidney disease risk, potassium optimization is a high-value target for anyone with blood pressure trending above optimal. If longevity is a priority, getting your potassium right is foundational – not optional.
Frequently Asked Questions
What potassium level is optimal for cardiovascular health?
Research consistently supports serum potassium between 4.0 and 5.0 mEq/L as optimal for cardiovascular health and arrhythmia prevention. The 3.5-4.0 mEq/L range, while technically “normal,” is associated with higher cardiovascular event rates in people with underlying heart disease. For longevity and performance, targeting the upper half of the reference range through dietary means is a worthwhile goal.
Can exercise affect potassium levels?
Yes, significantly. Intense exercise causes potassium to shift out of muscle cells into the bloodstream transiently – serum potassium rises during exercise and returns to normal within minutes of stopping. This transient rise is normal and does not indicate hyperkalemia. Prolonged exercise with significant sweating causes net potassium depletion over time, and athletes with high training volumes may have chronically lower potassium stores despite adequate serum levels – similar to the magnesium situation where serum levels are maintained at the expense of cellular stores.
Is potassium supplementation safe?
For healthy adults with normal kidney function, modest potassium supplementation (99-200 mg per day from OTC supplements) is generally safe. Higher doses – particularly prescription potassium chloride at 10-40 mEq per dose – are appropriate for treating documented deficiency under physician supervision. High-dose potassium is not safe without medical oversight in anyone with kidney disease, diabetes (especially with nephropathy), or anyone on ACE inhibitors, ARBs, or potassium-sparing diuretics. Cardiac arrest from hyperkalemia is a rare but real risk in vulnerable populations.
Why do my potassium levels fluctuate between tests?
Serum potassium fluctuates for several reasons: the timing of the draw relative to meals (potassium rises after eating), exercise before the draw (transiently raises potassium), prolonged tourniquet time or fist-clenching during blood draw (causes local potassium release from muscle), sample hemolysis (falsely elevates potassium dramatically), and normal day-to-day physiological variation. For a reliable baseline, potassium should ideally be drawn fasting in the morning without exercise immediately beforehand, and any unexpected result should be repeated before acting on it.
Low magnesium and low potassium – are they related?
Yes, and this is clinically important. Hypomagnesemia causes renal potassium wasting and makes hypokalemia resistant to treatment – you cannot effectively correct potassium deficiency without also correcting magnesium deficiency. When both are low, magnesium must be repleted alongside potassium for the potassium to normalize and stay normal. This is why checking magnesium alongside potassium in anyone with hypokalemia is standard clinical practice.
Testing Potassium With ApexBlood
Potassium is included in ApexBlood’s comprehensive metabolic panel alongside sodium, magnesium, kidney function markers, and the full metabolic picture that gives potassium the context it needs to be properly interpreted. If your potassium is outside optimal range, our physicians can discuss dietary strategies, identify potential causes including medication effects, and determine whether supplementation is appropriate based on your complete profile.
You cannot optimize what you do not measure. Potassium is one of the highest-leverage electrolytes for cardiovascular health, blood pressure, and athletic performance – and most people have no idea where theirs stands.
Get comprehensive testing for $189
The Bottom Line on Potassium
Potassium is the primary electrolyte inside your cells and one of the most powerful dietary modulators of blood pressure and cardiovascular risk available. The “normal” range masks meaningful performance differences – optimal potassium is in the upper half of the reference range, not just anywhere above 3.5 mEq/L. Most Americans consume far less potassium than they need, and this chronic insufficiency contributes to blood pressure elevation, muscle dysfunction, fatigue, and impaired cardiac rhythm stability.
Stop treating potassium as an afterthought. Optimize your dietary intake, monitor your levels, and understand how potassium interacts with sodium, magnesium, and kidney function to drive your cardiovascular health. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Potassium levels and electrolyte balance require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.