
Sodium is the primary electrolyte in your blood and extracellular fluid, and it is maintained within one of the narrowest ranges of any biomarker your body regulates. A serum sodium that deviates even a few millimoles per liter from normal can produce significant symptoms – from fatigue and cognitive impairment at mild deviations to seizures and coma in severe cases. But sodium’s clinical significance extends far beyond the emergency scenarios. Sodium status, hydration regulation, and the broader relationship between sodium, potassium, and aldosterone tell a nuanced story about your metabolic health, adrenal function, cardiovascular risk, and how well your body manages fluid balance under stress and during training. Most people dramatically oversimplify sodium to “salt is bad” – the reality is far more complex and more personally relevant than that narrative suggests.
What Is Serum Sodium?
Serum sodium measures the concentration of sodium ions in your blood plasma, expressed in milliequivalents per liter (mEq/L) or millimoles per liter (mmol/L). Sodium is the dominant cation (positively charged ion) in the extracellular fluid, and it is primarily responsible for regulating fluid distribution between the inside and outside of cells. Where sodium goes, water follows. The tight regulation of serum sodium is therefore inseparable from the tight regulation of blood volume and cell volume.
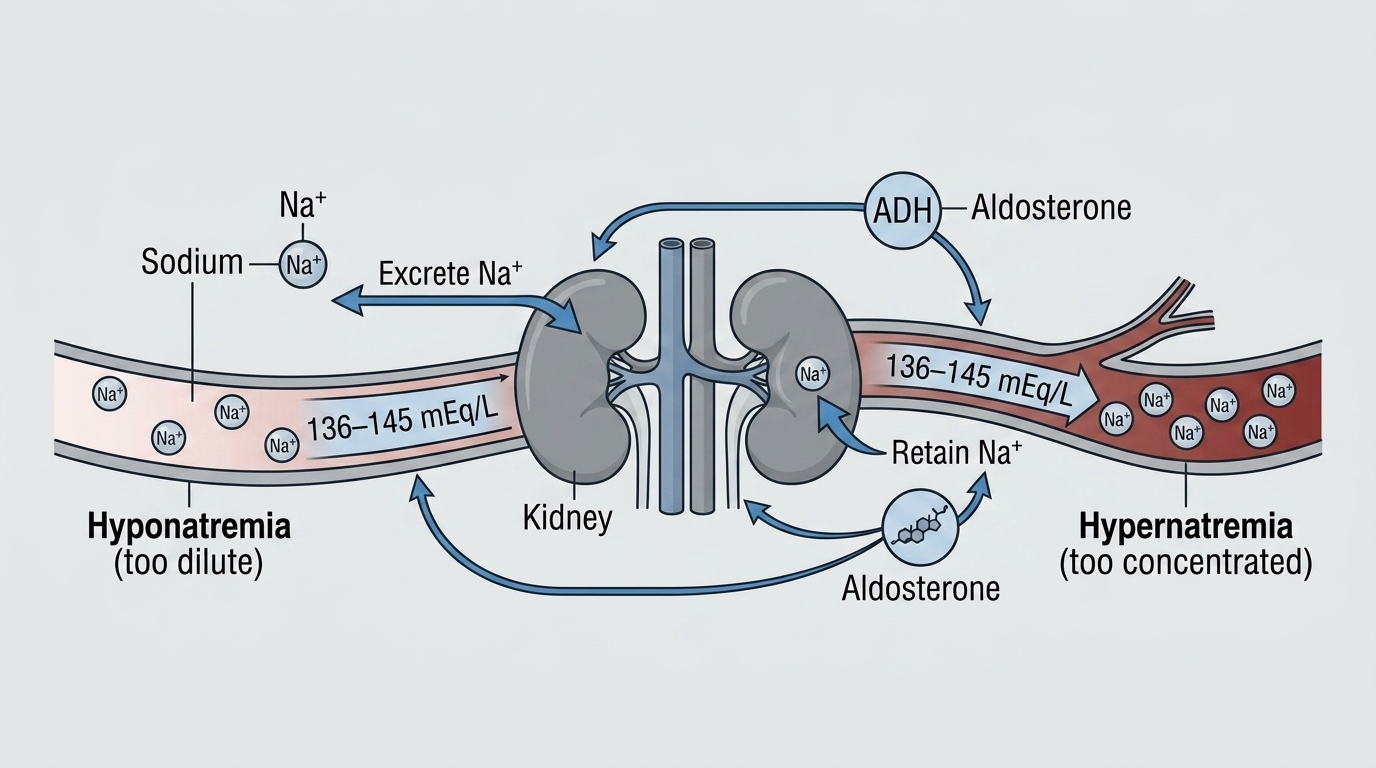
Sodium regulation involves a complex interplay of the kidneys, adrenal glands (through aldosterone), the hypothalamus and pituitary gland (through antidiuretic hormone/ADH), thirst mechanisms, and cardiac pressure receptors. When sodium is too high, the hypothalamus detects the increased osmolality, triggers thirst and ADH release, and the kidneys retain water to dilute the sodium concentration back to normal. When sodium is too low, ADH is suppressed, aldosterone acts to retain sodium, and the kidneys excrete free water to raise sodium concentration. This sophisticated system keeps sodium remarkably stable in most healthy people under normal conditions.
Why Sodium Matters for Performance and Health
Sodium is not just an electrolyte your doctor monitors during illness – it is a critical performance variable. Optimal sodium and hydration status affects muscle contraction efficiency, nerve signal transmission speed, blood pressure regulation, and cognitive function. Even mild hyponatremia (low sodium) – serum sodium at 130-134 mEq/L rather than the normal 135-145 mEq/L – measurably impairs cognitive performance, coordination, and exercise capacity. Athletes who develop exercise-associated hyponatremia (from drinking too much plain water without sodium replacement during endurance events) experience a cascade of symptoms from nausea and fatigue to, in severe cases, seizures and death.
On the other side, sodium restriction has been pushed as a universal cardiovascular intervention for decades – but the relationship between sodium intake and cardiovascular risk is genuinely more nuanced than “less is always better.” Salt sensitivity varies dramatically between individuals based on genetics, kidney function, and the renin-angiotensin-aldosterone system. For salt-sensitive individuals, high sodium intake raises blood pressure significantly. For salt-resistant individuals (roughly 50-60% of people), sodium intake has minimal blood pressure effects. Blanket low-sodium advice ignores this individual variation and in some cases produces worse outcomes – very low sodium intake activates the renin-angiotensin system in ways that may be independently harmful.
Normal vs. Optimal Sodium Levels
Standard Reference Ranges: Most laboratories report serum sodium as normal between 135 and 145 mEq/L (or mmol/L). Below 135 mEq/L is hyponatremia. Above 145 mEq/L is hypernatremia. These ranges are physiologically validated – outside these bounds, cellular function becomes genuinely impaired, and the risk of serious neurological symptoms rises significantly.
The Optimal Zone Within Normal: Unlike many biomarkers where the reference range is too broad to be meaningful for optimization, sodium’s tight regulation means that most healthy adults will naturally maintain levels in the 138-143 mEq/L range without much intervention. Values consistently toward either extreme of the reference range – low-normal (135-137 mEq/L) or high-normal (143-145 mEq/L) – may warrant investigation of the underlying regulatory physiology rather than direct sodium manipulation. Low-normal sodium should prompt evaluation of fluid intake patterns, cortisol and aldosterone function, thyroid status, and medication effects. High-normal sodium often reflects mild dehydration or inadequate fluid intake.
Performance Optimization: For athletes, the practical sodium optimization question is not serum sodium but rather appropriate sodium intake relative to sweat losses during training. Heavy sweaters – those who produce salty sweat (white residue on skin and clothing after exercise) – have elevated sodium losses that must be replaced to maintain hydration, electrolyte balance, and performance. These individuals often do not consume enough sodium to replace what they lose, leading to performance-degrading hyponatremia during prolonged training or competition.
What Causes Low Sodium (Hyponatremia)?
Hyponatremia has many causes that fall into three categories based on body fluid status. Hypovolemic hyponatremia occurs when both sodium and water are lost but water is replaced without sodium – the classic endurance athlete scenario, or vomiting and diarrhea with only water replacement. Euvolemic hyponatremia (most common overall) occurs when water is retained without sodium retention – causes include SIADH (syndrome of inappropriate ADH secretion from brain injury, lung disease, certain medications, or tumors), hypothyroidism, adrenal insufficiency, and excessive plain water intake. Hypervolemic hyponatremia occurs when both sodium and water are retained but proportionally more water – in heart failure, cirrhosis, and kidney disease. Medications are a major cause of hyponatremia – diuretics (especially thiazides), SSRIs/SNRIs, and many other drugs can disrupt sodium regulation. Identifying the type of hyponatremia is essential for proper treatment – giving sodium to someone with SIADH will not fix the problem.
What Causes High Sodium (Hypernatremia)?
Hypernatremia is almost always a problem of inadequate fluid intake or excessive fluid losses – the sodium concentration is high because there is not enough water. The most common cause in outpatients is simple dehydration – not drinking enough fluid to keep pace with losses from sweat, respiration, and urine. Diabetes insipidus (central or nephrogenic) causes excessive urinary water losses, producing hypernatremia despite intact thirst. Very high sodium intake without adequate water can produce hypernatremia but is rare in healthy people with normal thirst. Elderly people with impaired thirst sensation are at highest risk for dehydration-driven hypernatremia.
Sodium, Blood Pressure, and Cardiovascular Risk
The relationship between sodium intake and blood pressure is real but highly variable between individuals. The DASH-Sodium trial and numerous others confirm that reducing sodium from high (3,300+ mg/day) to lower levels (1,500-2,300 mg/day) reduces blood pressure in salt-sensitive individuals by 4-8 mmHg systolic – meaningful but not dramatic. In salt-resistant individuals, the same reduction produces minimal blood pressure change. Knowing whether you are salt-sensitive – ideally through blood pressure monitoring across different sodium intake periods – is more useful than applying a blanket recommendation. Importantly, the sodium-to-potassium ratio may matter more for blood pressure and cardiovascular risk than absolute sodium intake. Most Americans have an inverted ratio (much more sodium than potassium) due to processed food dominance. Increasing potassium intake alongside monitoring sodium produces better cardiovascular outcomes than sodium restriction alone.
Frequently Asked Questions
Should athletes eat more sodium?
Many athletes – particularly heavy sweaters doing prolonged endurance training – yes. Sweat contains significant sodium, and replacing only water after high-sweat-rate exercise dilutes serum sodium, impairing performance and (in extreme cases) causing hyponatremia. Sports drinks with sodium, adding salt to food, and using electrolyte supplements during prolonged exercise are all reasonable strategies for athletes with high training volumes. The appropriate sodium level is individual and depends on sweat rate, training duration, and climate conditions.
Is dietary sodium as harmful as commonly stated?
The evidence is more nuanced than popular messaging suggests. For salt-sensitive individuals (estimated at 40-50% of people with hypertension and 25-30% of normotensives), reducing sodium does meaningfully lower blood pressure and likely reduces cardiovascular risk. For salt-resistant individuals, the benefit is much smaller. Very low sodium intake (below 1,500 mg/day) activates the renin-angiotensin-aldosterone system and raises insulin resistance markers in some people, potentially causing harm in certain populations. The PURE study found a J-shaped curve – both very low and very high sodium intake were associated with worse outcomes compared to moderate intake (3,000-5,000 mg/day).
What causes serum sodium to be slightly low-normal?
Persistently low-normal sodium (135-137 mEq/L) warrants investigation rather than dismissal. Common causes include subclinical SIADH from medications (SSRIs are particularly common offenders), mild hypothyroidism, subclinical adrenal insufficiency, excessive fluid intake relative to sodium, and mild heart or kidney dysfunction. If you are regularly mildly hyponatremic on blood work, a thorough medication review and evaluation of thyroid and adrenal function is worthwhile before attributing it to lifestyle factors.
How does sodium interact with potassium?
Sodium and potassium are the yin and yang of cellular electrolyte balance. The sodium-potassium ATPase pump maintains the electrochemical gradient across cell membranes that drives nerve transmission, muscle contraction, and glucose transport. High sodium relative to potassium – the dominant pattern in processed-food diets – is associated with higher blood pressure and cardiovascular risk independent of absolute sodium intake. Increasing potassium through fruits, vegetables, and legumes while moderating processed food sodium is a more impactful strategy than sodium restriction alone.
Can sodium affect cognitive performance?
Yes. Even mild hyponatremia in the 130-134 mEq/L range measurably impairs cognitive performance, attention, and reaction time – well above the threshold for clinical symptoms like nausea and headache. Studies in elderly populations show that mild chronic hyponatremia is associated with increased fall risk and cognitive decline. Optimal hydration and sodium status supports peak cognitive function, and dehydration-driven hypernatremia similarly impairs concentration and mood.
Testing Sodium With ApexBlood
Sodium is included in ApexBlood’s comprehensive metabolic panel alongside potassium, chloride, bicarbonate, kidney function, and glucose – giving you the complete picture of your electrolyte balance and metabolic health. Sodium in context with your other electrolytes, aldosterone-related markers, and kidney function allows for accurate interpretation of what is driving any abnormality and what the appropriate response is.
You cannot optimize what you do not measure. Understanding your complete electrolyte status is the foundation for intelligent hydration strategies and cardiovascular health optimization.
Get comprehensive testing for $189
The Bottom Line on Sodium
Sodium is not the simple villain of cardiovascular disease it has been made out to be, nor is it irrelevant to health – the truth is more individual and more nuanced. Serum sodium tells you whether your fluid-electrolyte regulatory system is working and whether you are adequately hydrated. The most performance-relevant questions are often not serum sodium on a blood panel but rather whether your sodium and fluid replacement strategies during training match your actual needs, and whether your sodium-to-potassium ratio in daily nutrition supports rather than undermines your cardiovascular health.
Test comprehensively. Understand your complete electrolyte picture. Stop accepting oversimplified “eat less salt” advice when your individual biology may require a more nuanced approach. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Sodium levels and electrolyte balance require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.