
Most people have never heard of TIBC. If they have, they were probably told it was “fine” without any explanation of what it actually measures or why it matters. Total Iron Binding Capacity is one of the most useful tests for understanding your iron status – not just whether you are deficient, but why you are deficient and how severe the depletion actually is. Ferritin alone tells you how much iron you are storing. TIBC tells you how desperately your body is reaching for more.
What Is TIBC?
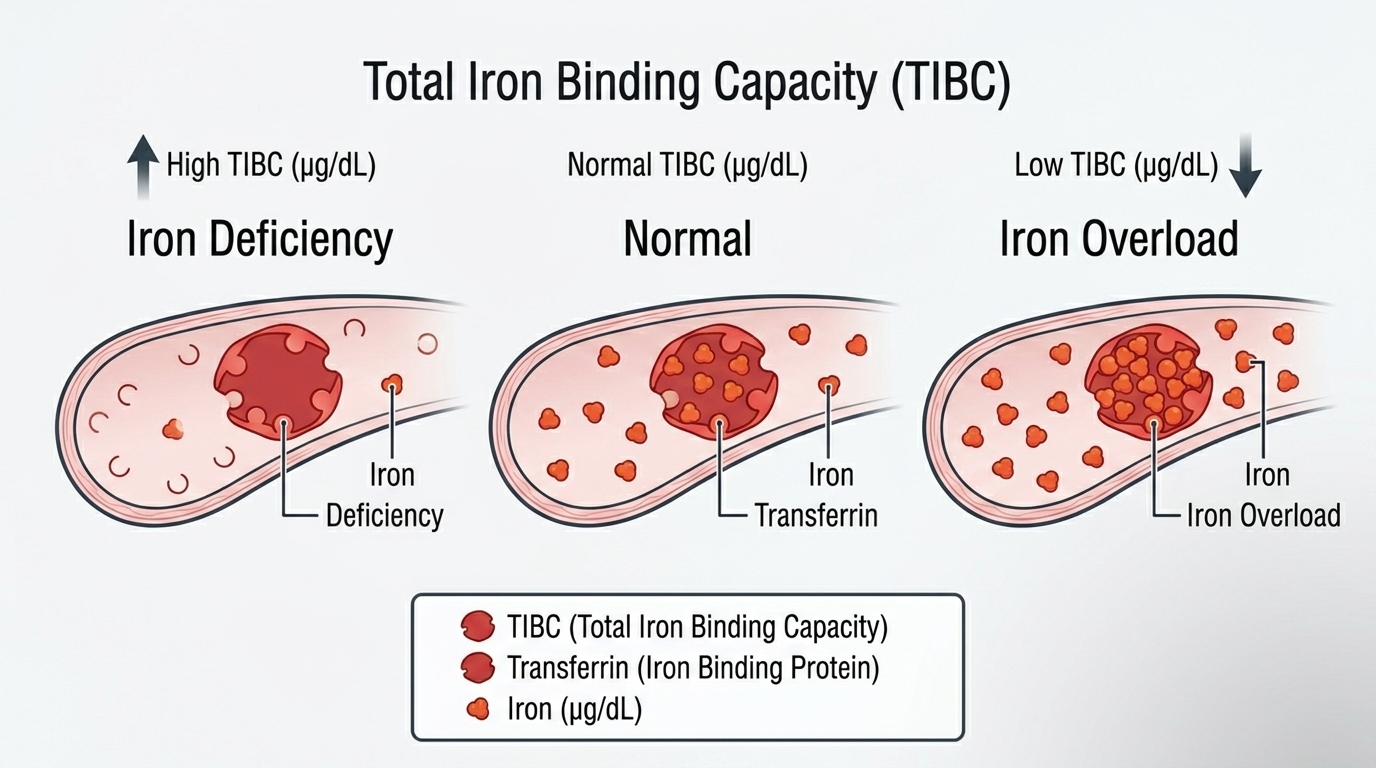
Total Iron Binding Capacity measures the maximum amount of iron that your blood could carry if every available binding site on transferrin were occupied. Transferrin is the protein that transports iron through your bloodstream – think of it as the delivery truck, and TIBC measures the total capacity of all those trucks combined. When iron stores are low, your liver produces more transferrin to capture every available iron molecule. When iron stores are adequate or excessive, transferrin production decreases because there is less demand.
TIBC is not a direct measurement of transferrin – it is a functional test of how much iron your blood could theoretically bind. It is calculated by adding serum iron (the iron actually bound to transferrin right now) to UIBC (the unoccupied binding capacity available to grab more iron). Together, these numbers give you a complete picture of your iron transport system: how much iron is being moved, how much capacity is available, and how efficiently the system is operating.
Why TIBC Matters for Performance and Health
TIBC matters because it provides crucial context that ferritin alone cannot give you. Iron deficiency exists on a spectrum, and TIBC helps identify where you fall. In the earliest stage of iron depletion, ferritin drops but TIBC has not yet risen significantly. As iron depletion progresses, TIBC rises as the body upregulates transferrin production to capture whatever iron is available. In frank iron deficiency anemia, you typically see very low serum iron, very high TIBC, low ferritin, and low hemoglobin together.
TIBC also helps distinguish between different types of anemia. Iron deficiency anemia shows high TIBC. Anemia of chronic disease (caused by inflammation rather than true iron depletion) typically shows low or normal TIBC despite low iron – because inflammation suppresses transferrin production as part of the acute phase response. Getting this distinction right matters enormously: treating inflammation-driven anemia with iron supplementation is ineffective and potentially harmful. TIBC is a key part of getting that distinction right.
Normal vs. Optimal TIBC Levels
Standard Reference Ranges: Most laboratories report TIBC as normal between 250 and 370 mcg/dL (micrograms per deciliter). Some labs use slightly different units (like mcmol/L) but the clinical interpretation is the same. These ranges reflect population averages and are designed to identify clear abnormalities rather than optimize iron transport efficiency.
The Problem With “Normal”: A TIBC of 260 mcg/dL and a TIBC of 360 mcg/dL are both “normal” by standard reference ranges. But they tell very different stories depending on context. TIBC at the high end of normal, combined with low-normal ferritin and low-normal serum iron, may indicate early iron depletion that is not yet severe enough to be flagged as abnormal – but is already affecting energy levels, recovery, and cognitive performance. Context and trend matter more than any single number.
Optimal TIBC for Performance: For most metabolically healthy adults with adequate iron stores, TIBC should fall in the middle of the reference range – roughly 280 to 340 mcg/dL. TIBC consistently above 360 mcg/dL suggests the body is reaching for more iron and may indicate depleting stores worth addressing. TIBC below 250 mcg/dL – particularly if ferritin is elevated – may indicate iron overload, chronic disease, liver disease, or malnutrition. The number only becomes meaningful when interpreted alongside serum iron, ferritin, and transferrin saturation.
What High TIBC Means
Elevated TIBC is the body’s distress signal for iron. When TIBC is high, your liver is producing more transferrin in an attempt to capture iron from whatever sources are available. This upregulation happens in response to iron deficiency – the body recognizes that iron delivery is insufficient and increases transport capacity to compensate. High TIBC accompanied by low ferritin and low serum iron confirms iron deficiency. High TIBC with low serum iron but normal ferritin may indicate functional iron deficiency, early depletion, or a more complex pattern requiring further investigation. High TIBC during pregnancy is expected because iron demands increase substantially to support fetal development.
What Low TIBC Means
Low TIBC is more ambiguous and requires careful interpretation. When TIBC is low alongside high ferritin and high transferrin saturation, iron overload – potentially hereditary hemochromatosis – becomes a serious consideration worth investigating. The body reduces transferrin production when iron stores are abundant because demand is low. Low TIBC can also occur with chronic inflammatory disease, liver disease (because the liver produces transferrin and diseased livers produce less), malnutrition or protein deficiency, and kidney disease. Low TIBC from inflammation looks different from low TIBC from iron overload – your serum iron and ferritin help tell those stories apart.
How to Interpret TIBC With Other Iron Markers
TIBC is most powerful when read alongside the rest of your iron panel. The classic iron deficiency pattern shows low ferritin, low serum iron, high TIBC, and low transferrin saturation (typically below 20%). The classic iron overload pattern shows high ferritin, high serum iron, low TIBC, and high transferrin saturation (typically above 45-50%). Anemia of chronic disease typically shows low serum iron, low or normal TIBC, and normal or high ferritin – because inflammation sequesters iron inside storage proteins rather than allowing it to circulate. Understanding which pattern applies to your results determines the appropriate response. The wrong treatment based on incomplete information – such as supplementing iron when inflammation is the real driver – can be counterproductive and even harmful.
What Affects TIBC?
Iron status is the primary driver of TIBC, but several other factors influence it. Pregnancy raises TIBC as iron demands increase. Inflammation and acute illness lower TIBC as the body reduces transferrin as part of the acute phase response – the same response that elevates ferritin. Liver disease reduces TIBC because transferrin is produced in the liver. Malnutrition and protein deficiency lower TIBC because transferrin is a protein. Estrogen therapy can raise TIBC modestly. Oral contraceptives may also affect TIBC. These physiological influences mean that isolated TIBC changes must always be interpreted in the context of your complete health picture and medication list.
Frequently Asked Questions
What does a high TIBC mean for my iron status?
High TIBC typically means your body is producing extra iron transport capacity because iron stores are depleting and the body is trying to capture more iron from circulation. When elevated TIBC is combined with low ferritin and low serum iron, it confirms iron deficiency. The higher the TIBC relative to your serum iron, the more aggressively your body is reaching for iron it cannot find.
Can TIBC be normal even if I am iron deficient?
Yes. In early or mild iron depletion, TIBC may still fall within the normal range even though ferritin is declining. TIBC rises as iron depletion progresses – in early stages, ferritin may drop significantly before TIBC rises above the reference range. This is why ferritin is a more sensitive early indicator of iron depletion than TIBC alone. Looking at both together gives you a clearer picture.
What is the difference between TIBC and UIBC?
TIBC is the total iron-binding capacity – the maximum iron that could be bound if all transferrin sites were occupied. UIBC (Unsaturated Iron Binding Capacity) is the portion of that capacity that is currently unoccupied and available to bind more iron. The relationship is: TIBC = Serum Iron + UIBC. Transferrin saturation is then calculated as (Serum Iron / TIBC) x 100. All three numbers come from the same measurement and together tell the full iron transport story.
Does a low TIBC mean I have too much iron?
Low TIBC combined with high ferritin and high transferrin saturation raises concern for iron overload, and hereditary hemochromatosis should be on the differential. However, low TIBC can also occur with chronic inflammation, liver disease, kidney disease, and malnutrition – conditions that reduce transferrin production for reasons unrelated to iron overload. The full iron panel plus context from your other labs helps distinguish between these possibilities.
How does inflammation affect TIBC?
Inflammation lowers TIBC as part of the acute phase response – the same process that elevates ferritin and C-reactive protein. Transferrin is a negative acute phase reactant, meaning its production decreases when inflammation is active. This is why anemia of chronic disease (inflammation-driven) shows a different TIBC pattern than iron deficiency anemia. Recognizing this distinction prevents the clinical error of treating inflammatory anemia as iron deficiency.
Testing TIBC With ApexBlood
TIBC is included in ApexBlood’s comprehensive blood panel alongside serum iron, ferritin, transferrin saturation, and UIBC – giving you the complete iron status picture that makes each individual marker interpretable. A TIBC number in isolation is far less useful than understanding how it fits with the rest of your iron panel and metabolic markers. Our physicians interpret your complete picture rather than reacting to single numbers.
You cannot optimize what you do not measure. Understanding your full iron transport system is the first step toward addressing whatever is driving suboptimal levels.
Get comprehensive testing for $189
The Bottom Line on TIBC
TIBC is not a test that stands alone – it is a piece of a puzzle that only makes sense alongside serum iron, ferritin, transferrin saturation, and the clinical context of your health. High TIBC tells you your body is reaching for iron it cannot find. Low TIBC tells you either that iron is plentiful or that something – inflammation, liver disease, malnutrition – is suppressing transferrin production. Neither number means much without the full picture.
High performers do not guess at their biology. They test comprehensively, interpret accurately, and act on real data. Stop accepting partial panels when complete iron assessment is available. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Iron status and TIBC require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.