
TSH – thyroid stimulating hormone – is the master regulator of thyroid function and the single most important screening test for thyroid disease. Produced by the pituitary gland in the brain, TSH tells your thyroid gland how much thyroid hormone to make. When thyroid hormone levels are adequate, TSH stays low. When thyroid hormone is insufficient, the pituitary pumps out more TSH to stimulate greater production. This feedback loop makes TSH extraordinarily sensitive to thyroid function changes – often detecting thyroid dysfunction years before free T4 or T3 become abnormal. But here is what most people with “normal” TSH don’t know: there is a substantial difference between a TSH that keeps you out of the clinical disease range and a TSH optimized for peak cognitive function, metabolic health, and energy. That gap is where performance optimization begins.
What Is TSH?
TSH (thyroid stimulating hormone, also called thyrotropin) is a glycoprotein hormone produced by thyrotroph cells in the anterior pituitary gland. Its sole function is to regulate the thyroid gland. When TSH binds to receptors on thyroid follicular cells, it stimulates every step of thyroid hormone production: iodine uptake, thyroglobulin synthesis, thyroid peroxidase activity, and ultimately the production and release of thyroxine (T4) and triiodothyronine (T3).
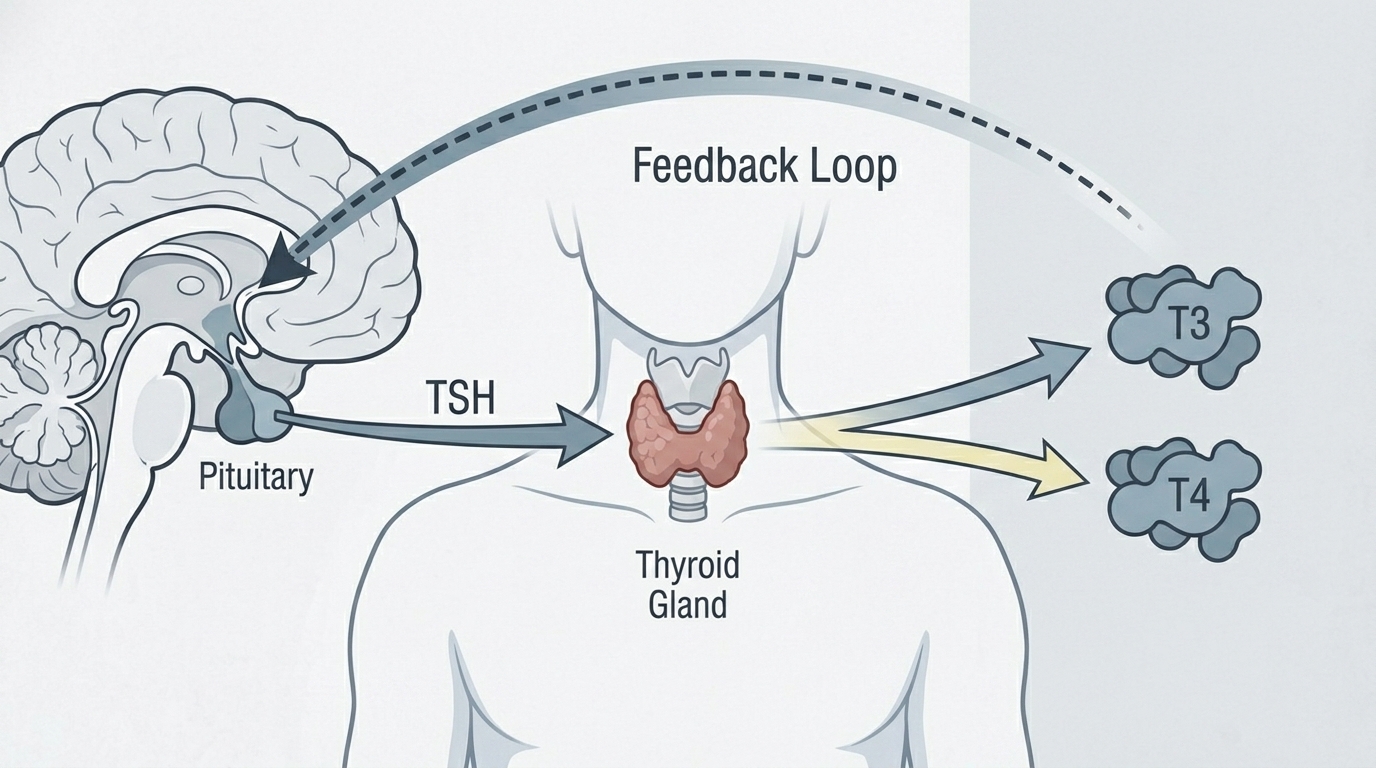
TSH is regulated through a classic negative feedback loop: the hypothalamus releases TRH (thyrotropin-releasing hormone), which signals the pituitary to release TSH. TSH stimulates the thyroid to produce T4 and T3. T4 and T3 then feed back to the pituitary and hypothalamus to reduce TRH and TSH release. This system maintains thyroid hormone levels within a remarkably tight range in healthy individuals. TSH is exquisitely sensitive to this feedback – a 50% change in thyroid hormone levels produces a much larger relative change in TSH (sometimes 10-fold or more), making TSH a sensitive amplifier of thyroid status.
Why TSH Matters for Energy, Metabolism, and Cognitive Performance
Thyroid hormone is the metabolic thermostat for virtually every cell in the body. T3 (the active form, converted from T4 in peripheral tissues) regulates basal metabolic rate, mitochondrial energy production, thermogenesis, heart rate, gut motility, cholesterol metabolism, bone turnover, and cognitive function. When thyroid hormone is optimal, you feel energized, mentally sharp, at a healthy body weight, with normal digestion, healthy cholesterol levels, and good mood and sleep. When thyroid hormone is suboptimal – even subtly – the consequences are diffuse: fatigue that sleep doesn’t fix, brain fog, difficulty managing weight despite appropriate diet and exercise, constipation, cold intolerance, depression, and impaired exercise recovery.
Hypothyroidism affects an estimated 20 million Americans, and approximately half of those with thyroid disease are undiagnosed. Subclinical hypothyroidism – TSH elevated above the upper reference range with free T4 still normal – affects an additional 4-8% of the population. Many more people have TSH within the “normal” reference range but at the higher end where symptoms of suboptimal thyroid function are common. Recognizing the difference between a TSH that is technically acceptable and one that supports peak function is central to thyroid health optimization.
Normal vs. Optimal TSH Levels
Standard Reference Ranges: The conventional laboratory reference range for TSH is approximately 0.5-4.5 mIU/L (some labs use 0.4-5.0 mIU/L). This wide range was established from population studies to capture approximately 95% of healthy adults. However, the reference population used to establish these ranges includes many individuals with subclinical thyroid dysfunction or undiagnosed thyroid disease, which may inappropriately widen the upper limit of what is called “normal.”
The Problem With “Normal”: A TSH of 4.0 mIU/L is within the laboratory reference range – but multiple studies show that TSH above 2.5 mIU/L is associated with higher LDL cholesterol, increased cardiovascular risk, cognitive symptoms, and a higher rate of progression to overt hypothyroidism over time. The American Association of Clinical Endocrinologists (AACE) has recommended that the upper limit of normal for TSH should be lowered to 2.5-3.0 mIU/L to better reflect optimal thyroid function. A large proportion of people with TSH in the 2.5-4.5 mIU/L range experience hypothyroid symptoms and may benefit from clinical evaluation and optimization.
Optimal TSH for Performance and Longevity: Longevity-focused physicians and functional medicine practitioners typically target TSH between 1.0 and 2.0 mIU/L as the optimal range for cognitive performance, metabolic health, and energy – while monitoring free T4 and free T3 to ensure adequate conversion and active hormone levels. Very low TSH (below 0.5 mIU/L) suggests hyperthyroidism or over-treatment with thyroid medication, which carries its own risks including cardiac arrhythmias, bone loss, and anxiety. The goal is precision within a narrower optimal window, not simply avoiding clinical disease.
What Causes High TSH (Hypothyroidism)?
Hashimoto’s thyroiditis (autoimmune hypothyroidism) is the most common cause of elevated TSH in developed countries – the immune system produces antibodies (TPO antibodies, thyroglobulin antibodies) that gradually destroy thyroid tissue, reducing thyroid hormone output and driving TSH higher. Iodine deficiency (the leading cause worldwide) reduces thyroid hormone synthesis. Surgical removal of the thyroid (thyroidectomy) for thyroid cancer or goiter requires lifelong thyroid hormone replacement. Radioactive iodine ablation for hyperthyroidism produces hypothyroidism as its intended effect. Medications including lithium, amiodarone, interferons, and certain checkpoint immunotherapy drugs can impair thyroid function. Radiation therapy to the neck for head and neck cancers damages thyroid tissue. Pituitary disease can cause secondary hypothyroidism (low TSH and low T4 together, rather than the high TSH of primary hypothyroidism).
What Causes Low TSH (Hyperthyroidism)?
Graves’ disease (autoimmune hyperthyroidism) is the most common cause of persistently low TSH – stimulating antibodies (TSI, thyroid stimulating immunoglobulins) bind TSH receptors and continuously activate thyroid hormone production independent of TSH. Toxic multinodular goiter contains autonomous thyroid nodules that produce thyroid hormone independently of TSH regulation. Toxic adenoma is a single autonomous nodule causing hyperthyroidism. Thyroiditis (viral, postpartum, silent) can cause a transient hyperthyroid phase as stored thyroid hormone is released from inflamed glandular tissue. Over-replacement with thyroid hormone medication is a common iatrogenic cause of suppressed TSH. Excessive iodine (from supplements, amiodarone, or iodinated contrast) can trigger both hyperthyroidism and hypothyroidism.
Hashimoto’s and the TSH Connection
Hashimoto’s thyroiditis deserves specific attention because it is the most common autoimmune condition in the United States and because its relationship with TSH is often misunderstood. Hashimoto’s is confirmed by elevated TPO (thyroid peroxidase) antibodies and/or thyroglobulin antibodies. A patient with Hashimoto’s may have a normal TSH for years while autoimmune destruction is ongoing – the thyroid compensates by increasing output (driven by rising TSH) until enough tissue is destroyed that compensation fails and TSH rises clearly above normal. This means people with Hashimoto’s may feel hypothyroid symptoms at TSH levels still within the reference range, because their individual setpoint has been disrupted by ongoing immune attack. Treating to an optimal TSH target of 1.0-2.0 mIU/L rather than simply “within range” often improves symptoms substantially in Hashimoto’s patients.
Frequently Asked Questions
My TSH is “normal” but I feel exhausted. Could my thyroid still be the issue?
Yes. Many people with TSH in the 2.5-4.5 mIU/L range experience classic hypothyroid symptoms – fatigue, brain fog, weight gain, cold intolerance, constipation, dry skin, hair loss – while being told their thyroid is “fine” because TSH is within the laboratory range. Evaluation should include free T4 and free T3 (to assess active hormone levels), TPO antibodies (to detect Hashimoto’s), and assessment of symptoms in context. Many functional medicine and longevity physicians target TSH of 1.0-2.0 mIU/L as optimal, which would classify some people currently considered “normal” as candidates for treatment or closer monitoring.
What is the difference between TSH, T4, and T3?
TSH is the pituitary signal that tells the thyroid what to produce. T4 (thyroxine) is the primary hormone the thyroid secretes – it is relatively inactive itself. T3 (triiodothyronine) is the biologically active thyroid hormone that actually binds receptors in cells and drives metabolic effects. T4 is converted to T3 in peripheral tissues (liver, muscle, kidney) by enzymes called deiodinases. Problems can occur at any level: low TSH (pituitary dysfunction), low T4 despite normal TSH (rare primary thyroid production issue), or normal T4 but low T3 (impaired T4-to-T3 conversion, often from nutrient deficiency, stress, or chronic illness). A comprehensive thyroid assessment measures TSH, free T4, and free T3 to capture the complete picture.
Does diet affect thyroid function and TSH?
Yes, significantly. Iodine is required for thyroid hormone synthesis – deficiency causes goiter and hypothyroidism. Selenium is essential for the deiodinase enzymes that convert T4 to active T3 – deficiency impairs T4-to-T3 conversion and can cause elevated T4 with low T3. Zinc also supports thyroid hormone synthesis. Iron deficiency impairs thyroid peroxidase activity (the enzyme required for thyroid hormone production) and can worsen hypothyroidism in people with iron-deficient anemia. Very low-calorie diets and severe caloric restriction reduce T3 (the body adapts by slowing metabolism). Cruciferous vegetables (broccoli, cauliflower, kale) contain goitrogens that mildly inhibit thyroid function when eaten raw in large quantities – this is clinically relevant mainly in people with pre-existing iodine deficiency or thyroid disease.
How should TSH be interpreted in pregnancy?
Pregnancy significantly alters thyroid physiology and TSH interpretation. In the first trimester, high hCG (human chorionic gonadotropin) cross-activates TSH receptors and stimulates thyroid hormone production, causing TSH to fall – sometimes below the normal non-pregnant range. Pregnancy-specific TSH ranges apply: typically TSH 0.1-2.5 mIU/L in the first trimester, 0.2-3.0 mIU/L in the second, and 0.3-3.0 mIU/L in the third. Thyroid disease in pregnancy has significant implications for fetal brain development and pregnancy outcomes – all pregnant women should have TSH checked early in pregnancy, and women with Hashimoto’s or known hypothyroidism require more frequent monitoring.
Can stress affect my TSH and thyroid function?
Yes, through multiple mechanisms. Chronic physiological or psychological stress elevates cortisol, which suppresses TRH and TSH and impairs T4-to-T3 conversion. This is part of why people under prolonged stress often develop low T3 (the “low T3 syndrome” or “euthyroid sick syndrome”). Significant acute illness similarly suppresses thyroid hormones as part of the body’s adaptive response – measuring thyroid function during acute illness can give misleading results. Chronic stress also impairs the immune system in ways that may unmask or accelerate autoimmune thyroid disease in genetically susceptible individuals.
Testing TSH With ApexBlood
ApexBlood’s comprehensive panel includes TSH alongside free T4, free T3, and TPO antibodies – the complete thyroid assessment needed to evaluate not just whether your TSH is within the reference range, but whether your thyroid is producing and converting hormones optimally and whether autoimmune thyroid disease is present. Our physicians can discuss what your TSH means in the context of your symptoms, other metabolic markers, and personal health goals, and can guide optimization strategies for thyroid function.
Get comprehensive testing for $189
The Bottom Line on TSH
TSH is the most sensitive and specific single marker for thyroid function – the master signal that tells the entire thyroid system how hard to work. A TSH that keeps you out of the clinical disease range is not the same as a TSH optimized for energy, cognitive performance, metabolic health, and longevity. The optimal TSH window of 1.0-2.0 mIU/L – supported by growing evidence and adopted by leading functional medicine and longevity physicians – is narrower than the laboratory reference range and more relevant to how you actually feel and perform. Combined with free T4, free T3, and TPO antibodies, TSH becomes the cornerstone of a comprehensive thyroid assessment that can identify dysfunction years before it becomes obvious. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. TSH and thyroid function require evaluation by qualified healthcare providers. Never adjust thyroid medication without physician guidance. Always consult licensed medical professionals for diagnosis and treatment.