
UIBC – Unsaturated Iron Binding Capacity – is the portion of your iron transport system that is currently empty and available to carry more iron. It is the gap between what your blood could theoretically carry and what it is actually carrying right now. Most people have never been told what UIBC means even when it appears on their lab report, which is a significant oversight because UIBC provides immediate, actionable information about your iron status that complements ferritin and serum iron in ways neither marker can achieve alone.
What Is UIBC?
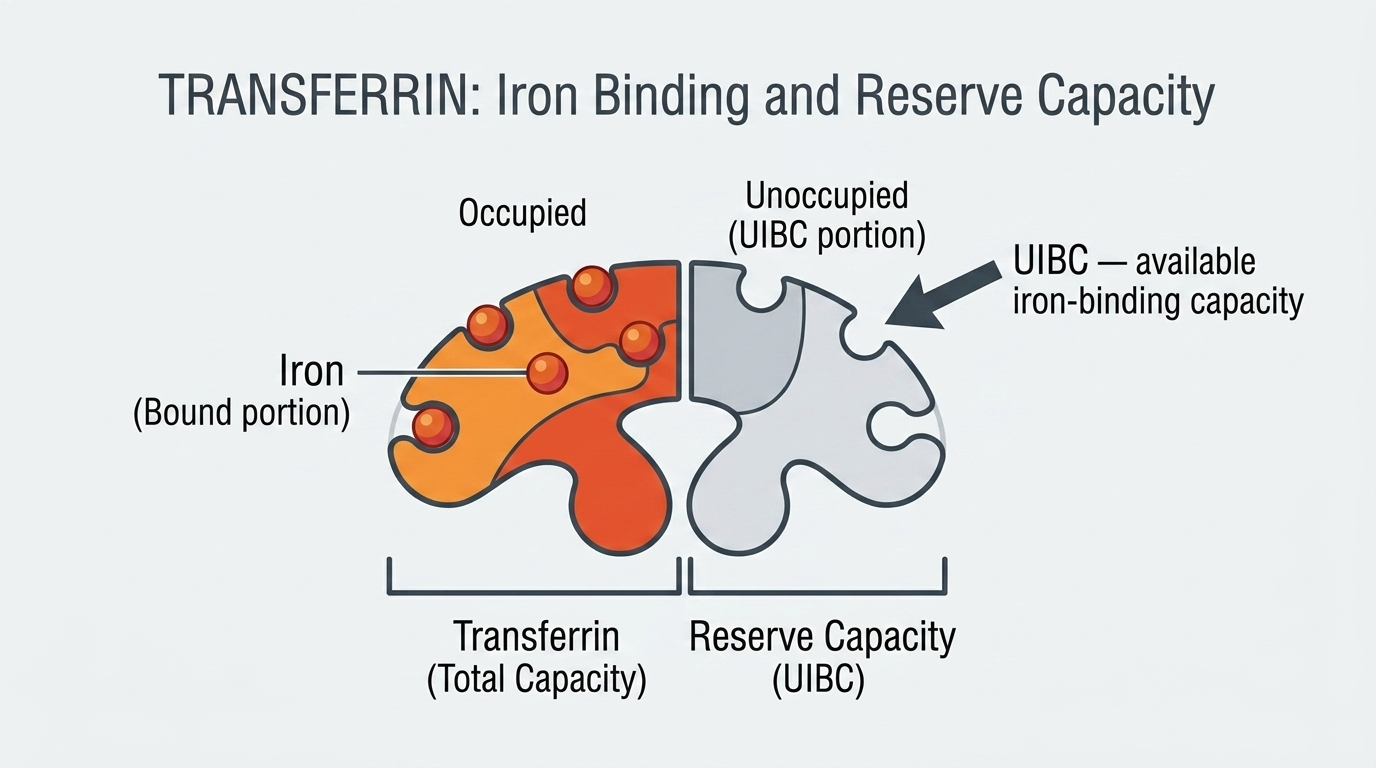
UIBC stands for Unsaturated Iron Binding Capacity. It measures the amount of unoccupied iron-binding sites remaining on transferrin – the protein responsible for transporting iron through your bloodstream. Think of transferrin molecules as delivery vehicles with multiple cargo slots. Serum iron tells you how many slots are currently filled. TIBC tells you the total number of slots available. UIBC tells you how many empty slots remain – how much additional iron your blood could pick up and transport if it were available.
The mathematical relationship is straightforward: UIBC = TIBC – Serum Iron. Transferrin saturation is then calculated as (Serum Iron / TIBC) x 100, expressed as a percentage. A high UIBC means many iron-binding sites are unoccupied – your transport vehicles are mostly empty, suggesting your body is not getting enough iron to fill them. A low UIBC means most sites are occupied – either iron is abundant or, in the case of iron overload, the transport system is saturated and iron is spilling into tissues where it causes damage.
Why UIBC Matters for Optimization
UIBC matters because it provides real-time information about iron transport efficiency that ferritin alone cannot give you. Ferritin reflects your long-term iron storage. UIBC reflects the current functional capacity of your iron delivery system. A person with declining ferritin but not yet dramatically low serum iron may show a rising UIBC before either of those markers reaches the “abnormal” flag level – giving you an earlier warning signal to act on.
For high performers, iron delivery efficiency matters enormously. Iron is not just stored – it needs to be actively transported to where it is needed: red blood cell production in bone marrow, mitochondrial energy production in muscle cells, enzymatic reactions throughout the body. When UIBC is high and transferrin saturation is low, it means iron is not flowing efficiently to these tissues regardless of what your ferritin says. Understanding this distinction is the difference between managing your biology proactively versus waiting for anemia to develop before acting.
Normal vs. Optimal UIBC Levels
Standard Reference Ranges: Most laboratories report UIBC as normal between 111 and 343 mcg/dL. Some labs report it in mcmol/L (multiply mcg/dL by 0.179 to convert). These reference ranges are, like most reference ranges, wide enough to include a broad population rather than define a target zone for optimal function.
The Problem With “Normal”: A UIBC of 120 mcg/dL and a UIBC of 330 mcg/dL are both “normal” by standard reference ranges. They reflect dramatically different iron delivery situations. High UIBC means your transferrin is largely empty – your iron transport capacity is mostly unused because there is not enough iron available to fill it. This is the hallmark of iron deficiency. Low UIBC means transferrin is nearly full – which may be appropriate when iron is adequate, or concerning when it indicates iron overload with transferrin saturation pushing above 45-50%.
Optimal UIBC for Performance: There is no universal “optimal” UIBC number because it must be interpreted alongside serum iron and ferritin. In general, for metabolically healthy adults with adequate iron stores, UIBC in the range of 150-250 mcg/dL alongside normal serum iron and ferritin in the 50-150 ng/mL range suggests a well-functioning iron delivery system. UIBC consistently above 300 mcg/dL alongside declining ferritin should prompt investigation and likely intervention. UIBC below 100 mcg/dL alongside high ferritin and high serum iron raises concern for iron overload.
What High UIBC Means
High UIBC is the physiological equivalent of your body broadcasting that it wants more iron. When UIBC is elevated, it means a large fraction of your transferrin molecules are traveling empty through your bloodstream, waiting to pick up iron that is not available. The body has upregulated transferrin production (reflected in elevated TIBC) to maximize iron capture efficiency, but there simply is not enough iron in circulation to fill those binding sites. High UIBC combined with low ferritin and low serum iron is the textbook iron deficiency pattern – the three markers tell one consistent story. High UIBC with normal ferritin but low serum iron suggests iron is stored but is not being released efficiently – which can occur with chronic inflammation blocking iron release from storage.
What Low UIBC Means
Low UIBC means most of your transferrin binding sites are already occupied. In the context of normal ferritin and normal serum iron, this may simply reflect adequate iron status. But low UIBC combined with high ferritin and high transferrin saturation is a warning sign for iron overload – the system is saturated, iron is spilling into circulation beyond transferrin capacity, and organ damage may be accumulating. Hereditary hemochromatosis, repeated blood transfusions, and excessive iron supplementation can all drive this pattern. Low UIBC can also occur with chronic inflammation or liver disease due to reduced transferrin production, independent of iron status. Distinguishing between these scenarios requires your full panel in context.
UIBC vs. Transferrin Saturation: Which Should You Track?
Both UIBC and transferrin saturation convey similar information but from different mathematical angles. Transferrin saturation (the percentage of binding sites occupied) may be more intuitive for many people – below 20% suggests iron deficiency, above 45-50% raises concern for iron overload. UIBC gives you the absolute number of unoccupied sites rather than a percentage. Neither is inherently superior – they are complementary. Some physicians prefer tracking transferrin saturation because it normalizes for individual variation in transferrin levels. Others find UIBC useful for monitoring trends over time. Your comprehensive panel should include both.
Frequently Asked Questions
What does a high UIBC indicate?
High UIBC typically indicates iron deficiency – your transferrin molecules are mostly empty because there is not enough iron available to occupy them. Combined with low ferritin and low serum iron, this is the classic iron deficiency pattern. Combined with normal ferritin but low serum iron, it may suggest functional iron deficiency where stored iron is not being effectively mobilized, often driven by chronic inflammation.
Is UIBC the same as TIBC?
No – they are related but distinct. TIBC is the total maximum iron-binding capacity of transferrin. UIBC is the portion of that capacity that is currently empty and available. The relationship is: TIBC = Serum Iron + UIBC. When you know any two of these values, you can calculate the third. Most comprehensive iron panels report all three alongside ferritin and transferrin saturation.
Can UIBC be low if I am iron deficient?
This would be unusual but can occur in certain circumstances. Chronic inflammatory conditions suppress transferrin production, which lowers TIBC and therefore UIBC – even in the presence of true iron deficiency. This is part of what makes anemia of chronic disease complex: the typical iron deficiency markers (high TIBC, high UIBC) may not appear because inflammation is suppressing transferrin. Ferritin in this setting is often normal or high despite functional iron deficiency in the tissues.
What transferrin saturation level is optimal?
For most adults, transferrin saturation between 25% and 40% represents a well-functioning iron delivery system with adequate stores. Below 20% suggests iron deficiency is affecting iron delivery. Above 45-50% raises concern for iron overload. The calculation – serum iron divided by TIBC, multiplied by 100 – can be done with any standard iron panel that includes both measurements.
How does UIBC change with iron supplementation?
As iron stores replete with supplementation, serum iron rises and UIBC falls – reflecting that more transferrin binding sites are now occupied as iron becomes available. You should see UIBC trending downward alongside rising ferritin and rising transferrin saturation as iron repletion progresses. Monitoring this trend every 8-12 weeks confirms that supplementation is working and helps identify the point when continued supplementation risks overshooting into excess.
Testing UIBC With ApexBlood
UIBC is reported as part of ApexBlood’s complete iron status panel alongside serum iron, TIBC, ferritin, and transferrin saturation. Each of these markers adds information the others cannot provide alone. Together they give you a complete and accurate picture of your iron storage, transport, and delivery efficiency – the foundation for understanding whether iron is actually reaching the tissues that need it for energy production, immune function, and performance.
You cannot optimize what you do not measure. A comprehensive iron panel gives you the precision to act on real data rather than guessing.
Get comprehensive testing for $189
The Bottom Line on UIBC
UIBC tells you how much of your iron transport capacity is sitting empty, waiting for iron that is not arriving. High UIBC is your body signaling iron hunger – the transport system is ready but the cargo is not there. Low UIBC may mean iron is plentiful or, if ferritin and serum iron are also elevated, that the system is overloaded. Neither extreme is optimal, and neither can be properly interpreted without the complete iron panel context.
Do not settle for partial information about your biology. Test comprehensively, understand what each marker means in context, and optimize based on the complete picture. Stop accepting “normal” when optimal is possible.
Medical Disclaimer: This information is for educational purposes and does not constitute medical advice. Iron status markers including UIBC require evaluation by qualified healthcare providers. Never make treatment decisions based solely on internet information. Always consult licensed medical professionals for diagnosis and treatment.